Peptide therapies are transforming functional medicine by targeting natural healing processes, immune modulation, hormonal balance, and more. Here's a quick overview of eight peptides gaining attention:
- BPC-157: Supports tissue repair and gut health. Used for injuries and inflammatory bowel conditions.
- TB-500 (Thymosin Beta-4): Aids in muscle, tendon, and cardiac tissue repair.
- Thymosin Alpha-1: Boosts immune function and helps manage chronic infections like Hepatitis B/C.
- CJC-1295 + Ipamorelin: Enhances growth hormone production for improved body composition and recovery.
- Sermorelin: Restores natural growth hormone secretion, addressing age-related declines.
- Melanotan II: Improves skin pigmentation and libido but requires careful monitoring.
- GHK-Copper: Promotes skin and hair regeneration, with applications in anti-aging and post-procedure recovery.
- Kisspeptin: Regulates reproductive hormones, with potential in fertility and sexual health treatments.
These peptides offer diverse clinical applications, but their use requires precise dosing, safety monitoring, and adherence to evolving regulatory guidelines. Below, we explore their mechanisms, benefits, dosing protocols, and safety considerations.
Benefits & Risks of Peptide Therapeutics for Physical & Mental Health
sbb-itb-7164bd9
1. BPC-157 for Musculoskeletal Healing and Gut Support
BPC-157 aligns with functional medicine's emphasis on supporting the body's natural ability to heal. This synthetic peptide, made up of 15 amino acids (1,419 Da), was originally derived from human gastric juice. Its structure allows it to remain stable in gastric acid for over 24 hours, making it effective for both oral and injectable use.
Mechanism of Action
BPC-157 works through the BPC157–FBXO22–BACH1 pathway, where it binds to FBXO22, stabilizing BACH1 and boosting proangiogenic factors like PDGFB, FGF2, FGFR1, and EGFR. It also activates the VEGFR2 pathway and the Akt-eNOS axis, increasing nitric oxide production.
"BPC157 drives angiogenesis through FBXO22-dependent stabilization of BACH1." - Cell Communication and Signaling
These processes promote fibroblast migration and collagen deposition, both critical for tissue repair. In rodent studies, BPC-157 improved microvascular density (from 1.7 ± 0.4 to 6.2 ± 3.2 vessels) and enhanced collagen fiber organization by reducing interfiber spacing (from 0.62 ± 0.21 μm to 0.18 ± 0.15 μm).
Key Clinical Applications
BPC-157 shows promise in two main areas:
Musculoskeletal Repair: Preclinical research highlights its ability to heal various injuries, including Achilles tendon tears, quadriceps muscle damage, tendon-to-bone repairs, and joint injuries. A 2021 pilot study by Lee and Padgett reported positive outcomes with intra-articular injections for knee pain. Additionally, a 2025 study by Lee and Burgess found intravenous infusions safe in healthy volunteers.
Gastrointestinal Support: In the digestive system, BPC-157 protects the esophagus, stomach, duodenum, and colorectal mucosa. It has been studied for conditions like gastric ulcers, inflammatory bowel disease, and intestinal permeability. Unlike NSAIDs, which can harm the gut lining, BPC-157 helps counteract NSAID-induced damage and stabilizes the gut barrier.
"BPC-157 demonstrates robust regenerative and cytoprotective effects in preclinical studies, positioning it as a potentially valuable tool in musculoskeletal medicine." - Flynn P. McGuire, Department of Physical Medicine & Rehabilitation, University of Utah
Dosing and Administration Considerations
For musculoskeletal injuries, subcutaneous injections (250–500 mcg/day) are recommended, while gastrointestinal conditions may benefit from oral doses (500–1,000 mcg/day).
| Condition | Route | Daily Dose | Cycle Length |
|---|---|---|---|
| Acute tendon/ligament injury | Subcutaneous | 500 mcg | 4–6 weeks |
| Chronic tendinopathy | Subcutaneous | 250–500 mcg | 8–12 weeks |
| Inflammatory bowel disease | Oral | 500–1,000 mcg | 8–12 weeks |
| Post-surgical recovery | Subcutaneous | 500 mcg | 4–6 weeks |
Reconstitute a 5 mg vial with 2 mL of bacteriostatic water, being careful not to shake the solution. Store it at 35–46°F and use within 2–4 weeks. For subcutaneous injections, use a 29–31 gauge insulin syringe and rotate injection sites (abdomen, thigh, or flanks) to avoid lipohypertrophy.
For soft-tissue injuries, combining BPC-157 with TB-500 can enhance healing by promoting both cell migration and angiogenesis.
Safety and Monitoring
BPC-157 is generally well-tolerated, with mild side effects like redness at the injection site, brief fatigue during the initial days, and occasional headaches. However, its ability to stimulate angiogenesis raises concerns about potential risks in individuals with active or recent cancer, as VEGF pathway activation could theoretically encourage tumor growth.
Two key regulatory considerations should be noted. First, the FDA has classified BPC-157 as a substance that may pose safety risks in compounding, listing it under the 503A Category 2 bulks list as of late 2023. Second, it is included on the WADA Prohibited List, meaning it is not allowed for competitive athletes subject to anti-doping regulations. Practitioners are advised to reassess patients at the 4-week mark, with noticeable improvements in function and pain reduction typically occurring between weeks 5 and 8.
This overview of BPC-157 highlights its potential, paving the way for further exploration of peptides that can broaden treatment options in functional medicine.
2. Thymosin Beta-4 and TB-500 for Tissue Repair
Tβ4 and its synthetic counterpart, TB-500, are widely recognized for their ability to aid in the repair of muscle, fascia, cardiac tissue, and even the cornea. The key difference between the two lies in their structure: Tβ4 is a naturally occurring, full-length peptide with 43 amino acids, while TB-500 is a synthetic fragment containing just 7 amino acids (Ac-LKKTETQ), specifically the actin-binding region (residues 17–23).
Mechanism of Action
Tβ4 primarily works by binding to G-actin, facilitating rapid cell movement to areas of injury. This mechanism is crucial for wound healing and tissue remodeling.
But Tβ4 does much more than actin regulation. It stimulates VEGF to promote blood vessel growth, reduces inflammation by inhibiting NF-kB (targeting cytokines like TNF-α and IL-1β), and activates the ILK-Akt pathway to protect heart cells from programmed cell death. Additionally, it is metabolized into Ac-SDKP, a fragment known for its anti-fibrotic properties, which helps limit scar tissue formation. These combined effects make Tβ4 highly versatile in clinical applications.
"Thymosin beta-4 is the first known molecule able to initiate simultaneous myocardial and vascular regeneration after systemic administration in vivo." - Deepak Srivastava, Gladstone Institutes
Key Clinical Applications
The unique roles of Tβ4 and TB-500 have made them valuable in various medical settings:
- Musculoskeletal injuries: Tβ4 and TB-500 are often used to treat injuries to tendons, ligaments, and muscles. They are frequently paired with BPC-157 for complementary action - Tβ4 focuses on actin binding, while BPC-157 enhances VEGF activity.
- Eye health: A Phase II trial of a 0.1% Tβ4 eye drop formulation (RGN-259) showed significant improvements in corneal staining and reduced discomfort in patients with dry eyes.
- Heart recovery: In a 2025 clinical trial involving 96 patients suffering from acute myocardial infarction, recombinant Tβ4 significantly reduced infarct size when administered within 8 hours of coronary intervention.
- Wound healing: Studies in rats demonstrated that topical Tβ4 accelerated wound closure by 42% compared to untreated controls.
Dosing and Administration Considerations
Treatment with Tβ4 typically follows a two-step protocol:
- Loading phase: 2–2.5 mg administered twice weekly for 4–6 weeks, either subcutaneously or intramuscularly.
- Maintenance phase: 2–2.5 mg given once weekly or every 10–14 days.
For eye-related treatments, a 0.1% topical solution applied multiple times daily is the standard.
Tβ4 has a subcutaneous bioavailability of 70–80%, with a plasma half-life of 4–6 hours for subcutaneous or intramuscular administration. Intravenous delivery results in a shorter half-life of around 2 hours. Proper storage is critical - reconstituted peptides must be refrigerated to prevent degradation.
Safety and Monitoring
Clinical studies have shown Tβ4 to be well-tolerated. Over 1,700 participants in trials using the ophthalmic formulation RGN-259 reported no serious drug-related adverse effects. Even at high doses - 1,260 mg daily for 14 days in IV studies - no toxicities were observed. Minor side effects include injection site irritation, mild fatigue, and occasional headaches.
While Tβ4's ability to promote blood vessel growth could theoretically support tumor vascularization in susceptible individuals, no animal studies have linked it to tumor initiation. From a regulatory perspective, Tβ4 is currently listed under the FDA Category 2 bulks list, limiting its use in standard 503A compounding. However, TB-500 is expected to move to Category 1 by early 2026, potentially increasing its availability through licensed compounding pharmacies. Both substances remain banned for competitive athletes under WADA's Section S2.
Before starting systemic Tβ4, it is advised to conduct baseline tests, including a CBC, comprehensive metabolic panel, and hs-CRP, to monitor inflammation and organ health throughout the treatment.
3. Thymosin Alpha-1 for Immune Modulation
Thymosin Alpha-1 (Tα1) stands out from peptides like Tβ4 and TB-500 due to its role in balancing immune function. Initially derived from thymic tissue and now synthesized in labs, Tα1 serves as a regulator of the immune system.
Mechanism of Action
Tα1 works by activating Toll-Like Receptors 2 and 9 (TLR2 and TLR9) in both myeloid and plasmacytoid dendritic cells. This activation sparks responses in both the innate and adaptive immune systems. It also supports immune health by encouraging lymphoid stem cells to develop into T-cell precursors and then mature into CD4+ helper T-cells and CD8+ cytotoxic T-cells, both critical for immune defense.
Key Clinical Applications
Tα1 has proven effective in treating chronic Hepatitis B and C. It's also used in oncology as an adjunct therapy, helping to restore immune function during chemotherapy or radiation treatments.
Dosing and Administration Considerations
The typical dose for Tα1 is 1.6 mg (or 0.8 mg/m²), delivered through subcutaneous injection.
| Indication | Frequency | Duration |
|---|---|---|
| Chronic Hepatitis B/C | Twice weekly | 6–12 months |
| Cancer adjuvant therapy | Twice weekly | 6–12 months |
| Acute immune support | As indicated | Short course |
Safety and Monitoring
Tα1 is generally well tolerated by patients. Regular monitoring is recommended to evaluate how well the treatment is working and to make any necessary adjustments. Its ability to modulate immune responses underscores its growing role in peptide-based therapies within functional medicine.
4. CJC-1295 With or Without Ipamorelin for Growth Hormone Support
CJC-1295 is a peptide that focuses on the growth hormone (GH) system. It's often paired with Ipamorelin in functional medicine to address age-related declines in GH and improve body composition.
How It Works
CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH). It binds to pituitary receptors, boosting the amplitude of GH pulses. There are two versions:
- No DAC (Drug Affinity Complex): Mimics natural secretion, with a short half-life of around 30 minutes.
- With DAC: Extends the half-life to 6–8 days by binding to albumin, compared to the native GHRH's brief 7-minute half-life.
Ipamorelin, on the other hand, works differently. As a selective ghrelin-receptor agonist, it increases the frequency of GH pulses through the Gq/calcium pathway. When combined with CJC-1295, which works via the Gs/cAMP/PKA pathway, the two produce a synergistic effect, resulting in 1.5–2 times more GH output.
"This combination yields a synergistic GH output exceeding the sum of individual effects." - Palmetto Peptides Research Team
One of Ipamorelin's standout features is its selectivity. Unlike other GH stimulators, it doesn’t significantly increase cortisol or prolactin levels. Together, these peptides are valuable for addressing adult growth hormone deficiency (AGHD) and improving body composition.
Primary Clinical Uses
This peptide combination is widely used in functional medicine for:
- Treating AGHD: Restores natural GH and IGF-1 secretion.
- Body Composition Improvements: Helps reduce visceral fat and boost lean muscle mass.
- Managing Somatopause: Addresses the natural decline in GH production with age.
When paired with other therapies like BPC-157, it offers a broader approach to patient care.
Dosing and Administration
Proper dosing is key to maximizing the benefits of CJC-1295 and Ipamorelin. A typical research protocol involves:
- Dosage: 100 mcg of CJC-1295 (No DAC) and 100 mcg of Ipamorelin per injection.
- Timing: Administer subcutaneously in a fasted state, 20–30 minutes before or after eating, to enhance the GH response.
For the No DAC version, some protocols suggest multiple daily injections, but a common approach is a single injection before bedtime to align with the body's natural GH cycle.
| Parameter | CJC-1295 (No DAC) | CJC-1295 (With DAC) |
|---|---|---|
| Half-Life | ~30 minutes | 6–8 days |
| Pattern | Pulsatile | Sustained elevation |
| Dosing Frequency | 1–3 times daily | Once weekly or biweekly |
| Best Use | Acute pulses with Ipamorelin | Long-term body composition protocols |
Peptide research cycles typically last 8–12 weeks, followed by a 4-week break to prevent receptor desensitization. For reconstitution, use bacteriostatic water (0.9% benzyl alcohol), gently swirl (do not shake), and store at 36–46°F (2–8°C). Reconstituted vials remain stable for up to 30 days when refrigerated.
Safety and Monitoring
Common side effects include mild reactions at the injection site (redness, swelling), flushing, headaches, and water retention. Since prolonged GH elevation can lead to mild insulin resistance, it’s important to monitor fasting glucose, insulin, and serum IGF-1 levels during treatment.
A noteworthy regulatory update occurred on February 27, 2026, when CJC-1295 was reclassified from FDA Category 2 to Category 1. This allows licensed compounding pharmacies to dispense it with a valid physician's prescription. However, caution is advised with the DAC version, as its clinical development was halted after a cardiovascular-related death in a Phase II trial. Ongoing reviews are assessing its long-term cardiovascular safety.
5. Sermorelin Acetate as a Growth Hormone Secretagogue
Sermorelin acetate is a well-known peptide used to support growth hormone (GH) production, aligning with the broader goal of restoring natural hormone balance - a recurring theme in peptide therapies. It has been available since 1997, when the FDA approved it under the brand name Geref for treating pediatric growth hormone deficiency. Although it was withdrawn in 2008 for commercial reasons, it can still be legally obtained through 503A compounding pharmacies.
Mechanism of Action
Sermorelin works by mimicking the active portion of natural growth hormone-releasing hormone (GHRH), stimulating GH release. It binds to GHRH receptors on somatotroph cells in the anterior pituitary, activating a cAMP/PKA signaling pathway. Importantly, sermorelin retains the body’s natural somatostatin feedback mechanism. When GH or IGF-1 levels become too high, the hypothalamus releases somatostatin to reduce GH production - something that exogenous GH therapy bypasses entirely.
"Sermorelin stimulates the pituitary gland to increase natural growth hormone production... preserving the body's hormonal feedback loops." - Mayo Clinic
Although sermorelin has a plasma half-life of just 10–20 minutes, its effects on GH secretion last 60–90 minutes. At standard doses, it does not significantly affect cortisol, prolactin, or ACTH levels, making it a cleaner option compared to other GH stimulators.
Key Clinical Applications
Sermorelin’s ability to restore natural GH secretion makes it versatile for various patient needs. One common use is addressing somatopause, the gradual decline in GH levels that begins around age 30 and decreases by about 14% per decade. In a 1997 study by Khorram et al., 19 participants aged 55–71 received a sermorelin analog nightly for 16 weeks. Male participants gained an average of 1.26 kg in lean body mass, along with improved insulin sensitivity and libido.
Sermorelin also proves helpful in combating muscle loss in patients taking GLP-1 receptor agonists like semaglutide or tirzepatide, which can accelerate muscle wasting during rapid weight loss. Sermorelin’s anabolic effects help counteract this risk. Additionally, it supports slow-wave (NREM) sleep by acting on sleep-regulating neurons in the hypothalamus, with many patients reporting better sleep quality within the first couple of weeks.
| Application | Primary Benefit | Target Population |
|---|---|---|
| Somatopause | Restores youthful GH levels | Adults 30 and older |
| GLP-1 Support | Prevents muscle wasting | Patients on semaglutide/tirzepatide |
| Sleep Optimization | Enhances slow-wave sleep | Individuals with age-related insomnia |
| Tissue Repair | Improves recovery and bone density | Athletes or post-injury patients |
These benefits highlight the importance of precise dosing strategies to achieve optimal results.
Dosing and Administration Considerations
For effective GH support, the typical adult dose is 200–300 mcg subcutaneously each night, administered on an empty stomach about 30–60 minutes before bed. A 2-hour pre-injection fast is recommended to improve receptor sensitivity. A common schedule is 5 days on, 2 days off (e.g., Monday through Friday) to maintain pituitary sensitivity and reduce the risk of desensitization. Treatment cycles generally last 8–12 weeks, followed by a 2–4 week break.
Sermorelin is also available as a buccal troche (600 mcg) or a nasal spray (approximately 100 mcg per spray), but subcutaneous injections remain the most commonly used method.
"Sermorelin represents a superior approach to managing adult-onset GH insufficiency compared with exogenous GH, because it preserves the pulsatile secretory pattern, maintains hypothalamic-pituitary feedback, stimulates pituitary gene transcription, and avoids tachyphylaxis." - Walker RF
Safety and Monitoring
Sermorelin has a strong safety record. The most common side effects are injection-site reactions, such as pain, swelling, or redness, reported in about 16.7% of patients in clinical trials. Some patients may also experience temporary facial flushing shortly after injection. These effects are usually mild and resolve on their own.
Monitoring focuses on serum IGF-1 levels, which should stay within the appropriate range for the patient’s age. Sermorelin is strictly contraindicated in individuals with active neoplastic disease, as elevated GH and IGF-1 levels could potentially promote tumor growth. Interestingly, in pediatric studies, anti-GHRH antibodies were detected in 78% of participants, but they did not impair growth velocity or GH response. As with other peptide therapies, baseline lab tests and ongoing monitoring are essential to ensure safe and effective treatment.
6. Melanotan II for Photoprotection and Libido
Melanotan II (MT-II) stands out among peptides for its diverse effects, ranging from skin pigmentation to sexual health. Despite its popularity in certain circles, MT-II has never been approved by the FDA and is classified as an unapproved research chemical. Its appeal lies in its ability to influence skin tone, sexual arousal, and appetite suppression, making it a subject of interest in anti-aging and functional medicine. Online interest in MT-II has surged, with a 208% increase in advertisements in 2024 and a 276% rise in marketplace sales over five years.
Mechanism of Action
MT-II is a synthetic analog of alpha-melanocyte-stimulating hormone (α-MSH), designed with a cyclic heptapeptide structure that makes it around 1,000 times more potent than natural α-MSH. Unlike Melanotan I (afamelanotide), MT-II can cross the blood-brain barrier, enhancing its effects. It acts as a broad-spectrum agonist, targeting melanocortin receptors MC1R, MC3R, MC4R, and MC5R.
- MC1R Activation: Promotes the production of eumelanin, offering protection against UV damage.
- MC4R Activation: Triggers central nervous system effects, such as sexual arousal and appetite suppression.
These combined actions explain MT-II's dual impact on photoprotection and libido.
"The appetite suppression and erectile effects that made MT-II popular... are not features - they are pharmacological proof of non-selective CNS receptor activation." - PeptideFox
Key Clinical Applications
MT-II's receptor-driven mechanisms make it noteworthy for two primary uses: skin protection and sexual health.
- Photoprotection: MT-II can enhance the Minimal Erythema Dose (MED) - a measure of UV tolerance - by 2–3 times baseline levels. While no formal clinical guidelines exist, this effect could benefit individuals with fair skin who are prone to UV damage.
- Sexual Health: Research has shown promising results for MT-II in addressing erectile dysfunction. In one study, 8 out of 10 men with psychogenic erectile dysfunction experienced noticeable improvements, with erections lasting an average of 38 minutes and achieving over 80% tip rigidity. Another trial found that a single 0.025 mg/kg dose enabled 85% of participants to achieve erections sufficient for intercourse. These findings contributed to the development of bremelanotide (PT-141), which was FDA-approved in 2019 for hypoactive sexual desire disorder in women.
Dosing and Administration Considerations
MT-II is typically administered through subcutaneous injections, though nasal sprays are available. However, the sprays often provide inconsistent absorption compared to injections.
| Phase | Dosage | Frequency |
|---|---|---|
| Titration/Tolerance Test | 100–250 mcg | Daily for 3–5 days |
| Loading | 250–500 mcg | Daily for 1–4 weeks |
| Maintenance | 500 mcg | 1–2 times per week |
| Sexual Health (Acute) | 250–500 mcg | Single dose 30–60 min before activity |
Doses are often taken in the evening, as nausea - MT-II's most common side effect - tends to peak 30–90 minutes after administration. Pre-dosing with an antihistamine may help mitigate nausea.
Safety and Monitoring
Compared to other peptides, MT-II is associated with a higher incidence of side effects. Nausea affects about 41% of users, increasing to 60–80% at doses of 0.16 mg/kg or higher. It can also raise systolic blood pressure (by 8–12 mmHg) and heart rate (by 10–15 bpm).
More severe adverse effects have been reported, including:
- Priapism: Prolonged erections lasting over 30 hours
- Rhabdomyolysis: Muscle breakdown requiring intensive care
- Renal Infarction: Damage to kidney tissue
MT-II's stimulation of melanocytes can lead to darker moles, the formation of new dysplastic nevi, and nail pigmentation changes. A baseline dermatological exam is essential, and individuals with a personal or family history of melanoma should avoid MT-II. Regular lab monitoring and clinical evaluations are crucial to ensure safety during treatment.
"MT-II is a biologically active, systemically acting peptide with limited human efficacy data, no robust long-term safety programme, and real-world evidence of serious adverse outcomes." - Peptide Science Thailand Editorial Team
7. GHK-Copper Peptide for Skin and Hair Regeneration
GHK-Cu is a peptide used in regenerative skincare that has gained attention for its ability to influence the expression of around 4,048 human genes - about 31.2% of the genome. Unlike many skincare ingredients that work through limited pathways, GHK-Cu operates at the genomic level, offering a broader range of effects. Levels of endogenous GHK-Cu naturally decline with age, dropping by about 60% from approximately 200 ng/mL at age 20 to around 80 ng/mL by age 60. This decline correlates with reduced skin elasticity and hair density.
Mechanism of Action
GHK-Cu works through two interconnected mechanisms. First, the GHK peptide itself alters gene expression, promoting skin repair by increasing the production of collagen (types I, III, and VI), glycosaminoglycans, and DNA repair genes while reducing inflammation through the downregulation of cytokines like IL-6 and TNF-α. Second, the copper ion (Cu²⁺) it delivers acts as a cofactor for essential enzymes like lysyl oxidase, which supports collagen and elastin cross-linking, and superoxide dismutase, which provides antioxidant protection. The copper ion also activates the Nrf2 pathway and enhances VEGF expression, aiding in wound healing and improving scalp blood flow.
"GHK-Cu works through two synergistic mechanisms: the GHK peptide activates gene expression changes... while the Cu²⁺ ion serves as a cofactor for lysyl oxidase and other copper-dependent enzymes critical for collagen and elastin cross-linking." - PeptideBond Editorial Team
Key Clinical Applications
The most well-documented uses of GHK-Cu are in anti-aging skincare and post-procedure recovery. In a study by Leyden et al., 67 women aged 41–62 used a GHK-Cu cream twice daily for 12 weeks. The results showed noticeable improvements in skin firmness, clarity, and elasticity, outperforming both a placebo and a Vitamin C cream. Another study on photoaging by Abdulghani et al. observed increased dermal thickness after 12 weeks of GHK-Cu application, as confirmed through histological analysis.
For post-procedure recovery, a 2024 study demonstrated that using a 0.05% GHK-Cu gel reduced epithelial recovery time by 25% and decreased inflammatory markers (IL-1β and TNF-α) by 30% following fractional laser resurfacing. This makes it a valuable option for accelerating healing after treatments like microneedling or chemical peels.
On the hair regeneration front, GHK-Cu has been shown to enhance follicle size, stimulate dermal papilla cell proliferation, and improve scalp circulation. Though minoxidil remains the gold standard for hair regrowth, GHK-Cu is increasingly used as a complementary treatment, especially for individuals who experience side effects from minoxidil.
Dosing and Administration Considerations
Topical application is the most evidence-supported route for GHK-Cu use. Injectable forms lack published human data on pharmacokinetics or efficacy, so practitioners should discuss this limitation with patients.
| Application | Route | Typical Concentration/Dose | Key Outcome |
|---|---|---|---|
| Anti-Aging | Topical | 0.01%–0.1% | Improved firmness, reduced wrinkles, increased dermal thickness |
| Post-Procedure Recovery | Topical | 0.05% gel | Faster epithelial recovery, reduced inflammation |
| Hair Growth | Topical | 1–10 µM (in vitro) | Increased follicle size, dermal papilla cell proliferation |
| Wound Healing | Subcutaneous | 0.5 µg per site (animal data) | Accelerated closure, increased tensile strength |
Important note: Avoid applying GHK-Cu alongside Vitamin C (ascorbic acid) in the same routine. Ascorbic acid can destabilize the copper ion, reducing the peptide's effectiveness. To maximize benefits, use Vitamin C in the morning and GHK-Cu in the evening. Consistent application for 8 to 12 weeks is typically required to see noticeable improvements in skin or hair quality.
Safety and Monitoring
GHK-Cu is generally well-tolerated. Studies show it is non-cytotoxic at concentrations up to 10⁻⁵ M (~4 µg/mL), and clinical trials have reported minimal side effects, such as irritation or dryness. Unlike retinoids, GHK-Cu does not increase photosensitivity.
However, it is contraindicated for individuals with copper metabolism disorders, such as Wilson's disease or Menkes disease, as these conditions impair copper regulation. Patients with active cancers should also use caution due to GHK-Cu's broad gene-modulating effects.
A regulatory update: as of February 27, 2026, GHK-Cu was reclassified from Category 2 to Category 1 on the FDA bulk drug substance list, making it legally available for compounding pharmacies with a physician's prescription. This change offers more flexibility for personalized treatment options.
8. Kisspeptin and Related Peptides for Reproductive Axis Modulation
Kisspeptin is often referred to as the master regulator of the reproductive axis. Unlike other peptides that typically act downstream, kisspeptin operates at the very top of the chain, making it a key player in addressing fertility, hormonal balance, and sexual health. This upstream role sets it apart in the realm of functional medicine.
Mechanism of Action
Kisspeptin’s mechanism underscores its potential in clinical settings. It binds to KISS1R (GPR54) receptors on GnRH-secreting neurons in the hypothalamus, triggering the pulsatile release of GnRH. This, in turn, prompts the anterior pituitary to release LH and FSH, which are essential for testosterone production in men and follicular development in women. The natural pulse generator for GnRH, located in the arcuate nucleus, fires every 60–90 minutes.
Kisspeptin works as part of the KNDy network alongside Neurokinin B (NKB), which stimulates, and Dynorphin (Dyn), which inhibits. It also integrates metabolic signals such as leptin and insulin, explaining why factors like extreme caloric restriction or very low body fat can completely suppress reproductive function.
"Without functional kisspeptin-GPR54 signaling, GnRH neurons do not fire, the pituitary receives no signal, and the gonads never activate." - Superpower
Key Clinical Applications
Kisspeptin-54 has shown promise as an IVF trigger. In a phase 2 trial involving 60 high-risk women, doses of 3.2–12.8 nmol/kg led to a 95% oocyte maturation rate with no cases of moderate to severe OHSS - an outcome that starkly contrasts with hCG triggers, which carry a 33.6 times higher risk of OHSS.
Beyond fertility treatments, kisspeptin is being explored for sexual health. A 2023 study by Mills et al. tested IV kisspeptin-54 (1 nmol/kg/h for 75 minutes) in 32 men with hypoactive sexual desire disorder (HSDD). The results? A 56% increase in penile tumescence compared to placebo (p=0.02), along with self-reported improvements in sexual satisfaction.
Other applications include its use as a diagnostic tool to differentiate between transient delayed puberty and permanent idiopathic hypogonadotropic hypogonadism (iHH). It’s also being studied as a marker for male infertility, with elevated serum kisspeptin levels in infertile men potentially offering greater sensitivity than FSH or LH alone.
Dosing and Administration Considerations
Kisspeptin requires parenteral administration - either subcutaneously or intravenously - because oral forms lack bioavailability. Two isoforms are commonly used:
| Isoform | Half-Life | Primary Use |
|---|---|---|
| Kisspeptin-10 (KP10) | ~4 minutes | Acute stimulation studies; pharmacokinetic research |
| Kisspeptin-54 (KP54) | ~28 minutes | IVF triggers; chronic dosing research; HSDD trials |
Daily dosing is avoided to prevent receptor desensitization, which could suppress testosterone levels to castration-like levels below 50 ng/dL. Instead, intermittent protocols - typically 2–3 times weekly - are preferred to maintain receptor sensitivity. A single injection can elevate LH levels 3 to 5 times above baseline within 2 to 5 hours.
As of 2026, kisspeptin is not FDA-approved for clinical use. It remains accessible primarily through academic research programs, reproductive endocrinologists, or specialized compounding pharmacies.
Safety and Monitoring
Kisspeptin has shown strong safety profiles in clinical trials, with no significant adverse effects reported at therapeutic doses. The main risk - axis suppression from overdosing - can be avoided with proper dosing schedules.
Before starting therapy, baseline labs (LH, FSH, testosterone/estradiol, SHBG, prolactin) should be established. Follow-up testing at weeks 4, 8, and 12 helps ensure the reproductive axis is functioning properly and detects early signs of desensitization. Kisspeptin therapy is not suitable for primary hypogonadism (testicular or ovarian failure), as stimulating the upstream signal has no effect when the gonads cannot respond.
Comparison Table
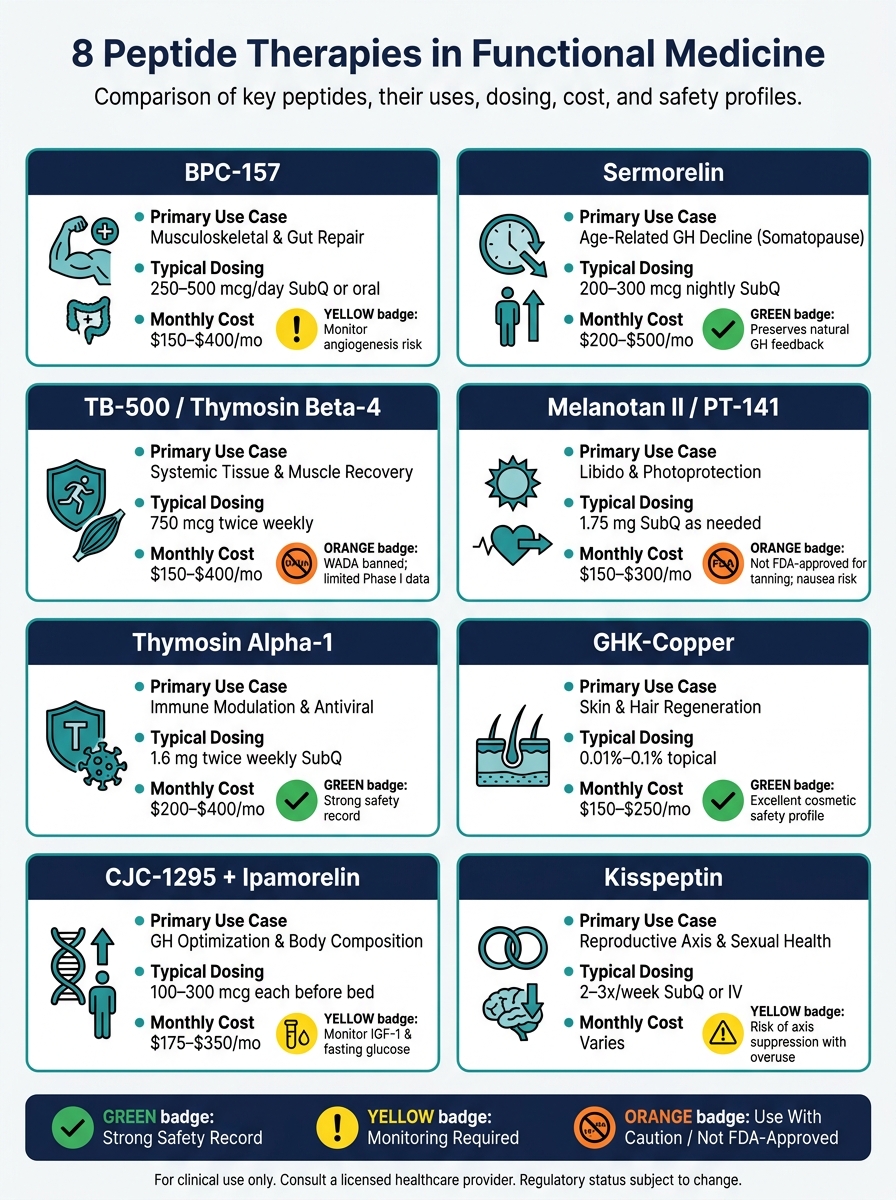
8 Peptide Therapies in Functional Medicine: Quick Comparison Guide
The table below provides an easy-to-digest overview of various peptides, highlighting their clinical applications, mechanisms, dosing guidelines, costs, and safety considerations.
| Peptide | Primary Use Case | Mechanism of Action | Typical Dosing | Monthly Cost | Key Safety Notes |
|---|---|---|---|---|---|
| BPC-157 | Musculoskeletal & gut repair | Activates VEGFR2 and nitric oxide pathways via the Akt-eNOS axis | 250–500 mcg/day (SubQ or oral) | $150–$400 | Potential tumor angiogenesis risk (theoretical) |
| TB-500 / Thymosin Beta-4 | Systemic tissue & muscle recovery | Actin-binding protein aiding cell migration to injury sites | 750 mcg twice weekly, 4–12 week courses | $150–$400 | Banned by WADA; limited Phase I safety data |
| Thymosin Alpha-1 | Immune modulation & antiviral support | Enhances T-cell differentiation and activates TLR9 | 1.6 mg twice weekly (SubQ) | $200–$400 | Mild injection site reactions; strong safety record |
| CJC-1295 + Ipamorelin | GH optimization & body composition | GHRH analog paired with a ghrelin receptor agonist | 100–300 mcg each, before bed | $175–$350 | Monitor IGF-1 and fasting glucose; watch for insulin resistance |
| Sermorelin | Age-related GH decline ("somatopause") | GHRH fragment (1–29) that directly stimulates the pituitary | 200–300 mcg nightly (SubQ) | $200–$500 | Maintains natural GH feedback mechanisms |
| Melanotan II / PT-141 | Libido & photoprotection | Acts on MC1R and MC4R, promoting CNS-mediated arousal | 1.75 mg SubQ, as needed (PT-141) | $150–$300 | Can cause nausea and transient hypertension; not FDA-approved for tanning |
| GHK-Copper | Skin & hair regeneration | Regulates ~31% of human genes, boosting collagen and DNA repair | 0.01%–0.1% topical or injectable per physician guidance | $150–$250 (injectable) | Excellent cosmetic safety; injectable forms face stricter regulatory oversight |
| Kisspeptin | Reproductive axis & sexual health | KISS1R agonist triggering GnRH → LH/FSH release | Intermittent SubQ or IV; 2–3×/week | Varies; available via specialized compounding | Risk of axis suppression with frequent use; not for primary hypogonadism |
This table serves as a practical guide for clinicians, offering a snapshot of how different peptides function and their potential applications.
For tissue repair, BPC-157 and TB-500 stand out, with BPC-157 also aiding gut health. In the realm of growth hormone therapies, CJC-1295 + Ipamorelin provides a potent combination for optimization, while Sermorelin takes a more conservative approach by preserving the body's natural feedback processes.
For anti-aging and cosmetic benefits, GHK-Copper shows impressive versatility, particularly in older patients. Meanwhile, Kisspeptin offers a targeted approach to reproductive health but requires precise dosing due to its less standardized protocols.
This summary equips practitioners with the insights needed to tailor peptide therapies to individual patient needs effectively.
Conclusion
The eight peptide therapies discussed here represent a growing area of interest in functional medicine. However, enthusiasm alone isn’t enough to establish effective clinical protocols. Each peptide operates through distinct biological mechanisms, has varying levels of evidence, and comes with important regulatory and safety considerations that healthcare professionals must carefully evaluate. Here's a quick recap of their specific roles:
- BPC-157 and TB-500: Both show promise in supporting tissue repair and recovery.
- Thymosin Alpha-1: The most well-documented option for immune system modulation.
- CJC-1295 with Ipamorelin and Sermorelin: Address age-related declines in growth hormone (GH) with complementary strategies, offering flexibility in treatment.
- GHK-Copper: Backed by strong evidence for topical applications.
- PT-141: FDA-approved for treating hypoactive sexual desire disorder (HSDD).
- Kisspeptin: Provides a targeted approach to reproductive health, though protocols are still being refined.
These therapies demand a structured and cautious clinical approach. As Dr. Lauren Leavitt, M.D., Co-Founder of Amanecia Health, emphasizes:
"Peptides are not a menu. They are medicine. The risks come from the wrong patient, the wrong dose, the wrong source, or the wrong combination."
To ensure safety and efficacy, practitioners should adhere to the following best practices: source peptides exclusively from FDA-registered, U.S.-based compounding pharmacies compliant with USP 797/795 standards, establish baseline laboratory evaluations before starting treatments, and introduce only one or two compounds at a time. Informed consent is critical, as many peptide therapies are compounded rather than FDA-approved for specific uses and carry potential long-term risks that remain uncertain.
The regulatory environment surrounding peptides is evolving rapidly. For example, as of April 22, 2026, twelve peptides previously categorized under the FDA's restricted Category 2 list were removed for further review, signaling ongoing regulatory changes. Staying informed about these developments is more than just good practice - it’s a professional obligation for clinicians.
FAQs
Which peptide should I choose for my patient’s primary goal?
The ideal peptide depends on the specific health goals of your patient. For tissue repair, gut healing, or injury recovery, peptides like BPC-157 and TB-500 are often chosen due to their regenerative abilities.
On the other hand, if the focus is on metabolic health, weight management, or anti-aging, options like GLP-1 receptor agonists (such as liraglutide or semaglutide) or growth hormone-releasing peptides like CJC-1295 and Ipamorelin may be more suitable.
Ultimately, the choice should always be tailored to the patient's unique needs and medical history to ensure the best possible outcome.
What baseline labs and follow-up monitoring are most important?
Baseline lab tests are crucial when starting peptide therapy. These typically include a comprehensive metabolic panel, IGF-1 (to assess growth hormone peptides), fasting glucose, HbA1c, and other relevant hormone or inflammatory markers.
For follow-up, IGF-1 levels are usually rechecked after 8–12 weeks, alongside periodic monitoring of fasting glucose and HbA1c during the course of therapy. This regular testing helps ensure both the safety and effectiveness of the treatment.
How do I stay compliant with FDA/WADA rules when prescribing peptides?
To ensure compliance, make sure the peptides you prescribe are either FDA-approved or legally compounded. Always document key details like informed consent, the clinical rationale for use, and your monitoring plans. Source peptides from licensed pharmacies that adhere to Good Manufacturing Practices (GMP). Avoid using research-only vendors, and stay informed about the latest FDA policies.
It's also important to follow state-specific regulations, maintain a valid physician-patient relationship, and avoid marketing peptides as performance enhancers or anti-aging treatments. These steps help protect both your practice and your patients.