
Short answer: I would not treat Epitalon as a proven anti-aging option. The article points to a familiar pattern: cell studies look strong, animal data look mixed but interesting, and human proof is weak.
If you want the fast take, here it is:
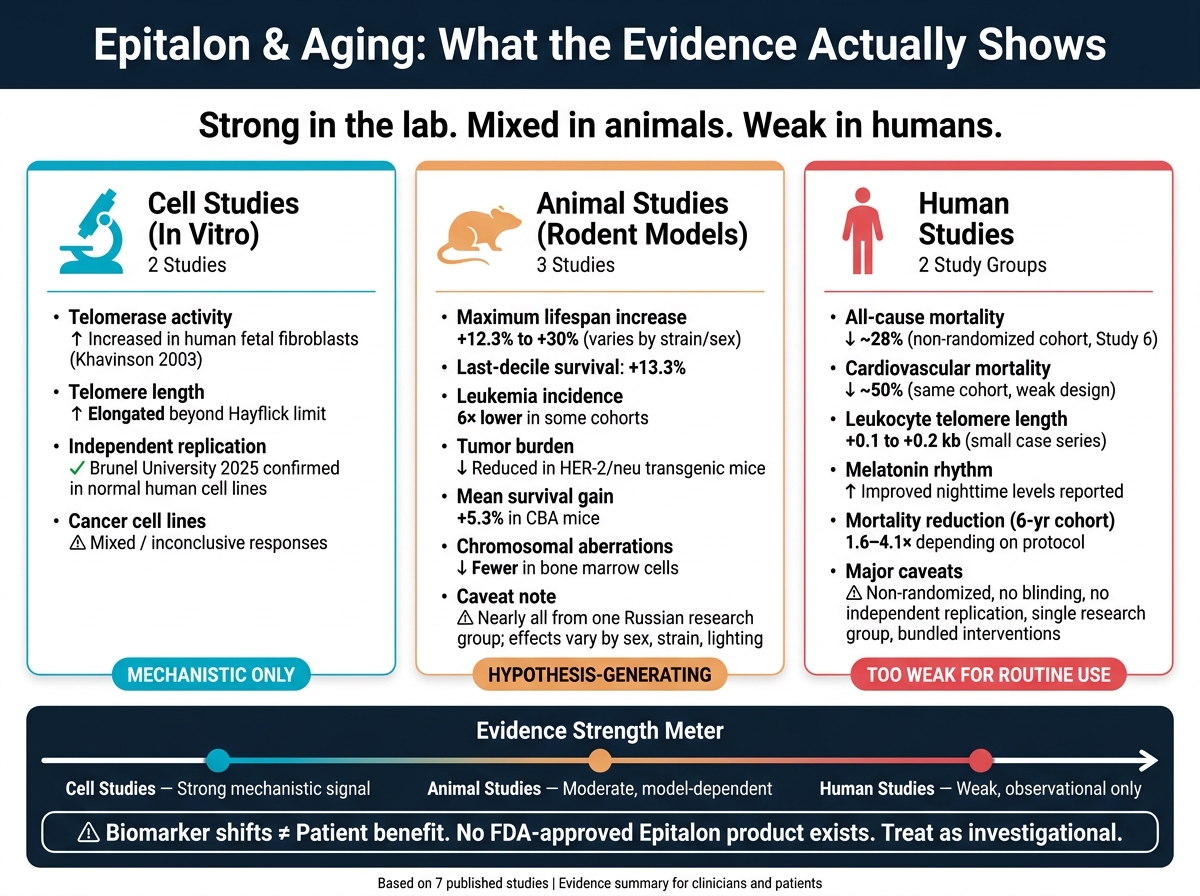
- 2 cell studies found higher telomerase activity and longer telomeres in lab-grown human cells.
- 3 animal studies linked Epitalon or epithalamin to longer maximum lifespan, fewer tumors in some models, and fewer chromosomal errors.
- 2 human study groups reported lower mortality, sleep and melatonin changes, and small leukocyte telomere gains.
- But the human work was mostly small, older, non-randomized, and from one research group.
- There is still no FDA-approved Epitalon product in the U.S.
- There is also a theoretical cancer concern because telomerase can support tumor growth.
So the big point is simple: biomarker shifts are not the same as patient benefit. A telomere change in a dish, or even in blood cells, does not prove longer life, better function, or safer aging in people.
Epitalon Research Evidence: Cell Studies vs. Animal Studies vs. Human Studies
Epitalon, Telomeres & Aging: What the Science Really Shows
sbb-itb-7164bd9
Quick comparison
| Study group | What it showed | How much weight I’d give it |
|---|---|---|
| Cell studies | Telomerase went up; telomeres got longer | Mechanism only |
| Animal studies | Some lifespan, tumor, and chromosome signals | Early support, not enough for care decisions |
| Human studies | Mortality and marker claims, but with weak design | Too weak for routine use |
My bottom line: the article supports more research, not routine prescribing (see our Epithalon clinical guide). If you’re reading this as a clinician or patient, the main takeaway is to separate lab promise from human proof.
Two human cell studies on telomere biology
These two in vitro studies help explain why Epitalon still gets attention at the mechanism level. They matter for a simple reason: they test the telomere idea before anyone starts talking about animal or human outcomes.
Study 1: Khavinson 2003 human fetal fibroblast telomerase study
Design and model: Khavinson's group exposed telomerase-negative human fetal lung fibroblasts to Epitalon over repeated passages, then measured telomerase, telomere length, and replicative lifespan.
Main findings: Epitalon increased telomerase activity, lengthened telomeres, and extended replicative lifespan beyond the expected Hayflick limit. That makes the mechanism look plausible. It does not show patient benefit. For a broader clinical overview of peptide therapy, practitioners should evaluate the underlying mechanisms alongside safety data.
Caveats: Fetal fibroblasts are a weak stand-in for aged adult tissue. There has been limited independent replication, the study is fully in vitro, and it says nothing about systemic exposure or cancer risk.
Study 2: 2025 Brunel University cell-line replication study
Design and model: This in vitro replication study tested Epitalon in normal human cell lines and cancer cell lines across multiple passages.
Main findings: In normal human cells, Epitalon increased telomere length, hTERT expression, and telomerase activity. Cancer-line responses were mixed. Again, this supports biologic plausibility, not patient benefit.
Caveats: This study is still in vitro only. And the mixed cancer-line response is a red flag that calls for caution in patient selection for those with known or occult neoplasia.
| Feature | Study 1: Khavinson 2003 | Study 2: Brunel University 2025 |
|---|---|---|
| Model | Telomerase-negative human fetal lung fibroblasts | Normal human cell lines plus cancer cell lines |
| Intervention | Epitalon across repeated passages | Epitalon across multiple passages with dose-response testing |
| Telomere outcomes | Telomere elongation and extended replicative lifespan beyond the Hayflick limit | Telomere length increases in normal cells; mixed effects in cancer lines |
| Telomerase outcomes | hTERT induction and increased telomerase activity | hTERT and telomerase increases in normal cells |
| Major limitations | Fetal cells are a poor proxy for aged adult tissue; same research group origin; purely in vitro | In vitro only; mixed cancer-line response raises theoretical oncologic concerns |
Taken together, these studies support biologic plausibility only. They do not prove clinical efficacy or human safety. The next step is to see whether this signal holds up in living organisms.
Three animal studies on lifespan, aging markers, and genomic stability
Animal studies carry more weight than cell studies, but the picture is still mixed. That matters for a simple reason: animals are the first real test of whether a telomere-related signal holds up outside a dish.
Study 3: Rodent lifespan extension in aged models
Design and model: Most lifespan data come from female mice and rats in Khavinson and Anisimov rodent studies. Treatment usually started in early adulthood. Epitalon was most often given subcutaneously in microgram doses, in short cycles, commonly 5 straight days per month.
Main findings: The clearest pattern shows up in maximum lifespan, not mean lifespan. In one SHR mouse study, maximum lifespan increased by 12.3%, and survival in the last decile improved by 13.3% compared with controls. Across several rodent strains, epithalamin and Epitalon were linked to maximum lifespan gains of about 10% to 30%. Some cohorts also reported a 6-fold lower leukemia incidence.
Caveats: Results changed by strain, sex, and housing conditions, with stronger effects in females. One rat study found stronger tumor inhibition under natural light than under standard lab lighting. Nearly all of this work comes from one Russian research group, with little independent replication in Western labs. So the lifespan signal is there, but it is still hard to map cleanly onto U.S. practice.
Study 4: Animal study on tumors, oxidative stress, or age-related pathology
Design and model: Several rodent studies tracked spontaneous tumor incidence, oxidative stress markers, and other age-related pathology in animals that received intermittent Epitalon or epithalamin courses.
Main findings: Treated animals had lower spontaneous tumor incidence, later tumor onset, and fewer chromosomal aberrations in bone marrow cells. Researchers took those changes as possible downstream aging effects tied to better genomic stability and less oxidative DNA damage. In one female CBA mouse study of pineal peptides, mean survival increased by 5.3%, maximum lifespan extended by 10 months, and researchers reported drops in body temperature, physical activity, free-radical processes, and spontaneous lung adenomas. In HER-2/neu transgenic mice, Epitalon did not significantly change mammary adenocarcinoma incidence, but it did reduce tumor burden, with more animals developing single tumors instead of multiple.
Caveats: The telomere link was indirect and not measured in a steady way. Pineal peptides may also act through endocrine, circadian, or immune pathways, and direct measurements of telomere length or telomerase activity in animal tissues are limited or reported unevenly. The next issue is whether those survival and tumor findings line up with measurable genomic stability.
Study 5: Animal study on genomic stability and telomere maintenance
Design and model: Some rodent studies looked past survival and asked whether Epitalon helps preserve chromosome integrity. These studies used chromosomal aberrations in bone marrow cells as a marker of genomic stability.
Main findings: Epitalon-treated animals showed fewer chromosomal aberrations and better karyotypic stability than controls. Some reviews also describe this through chromatin decondensation and related DNA repair hypotheses, which helps connect Epitalon, genome maintenance, and telomere biology.
Caveats: Direct in vivo telomere measurements are still sparse, older, and methodologically mixed. The genomic-stability signal makes sense, but the telomere mechanism is still unproven. Most of the strongest telomere-related evidence still comes from human cell culture, not rodent tissue assays. Even with that, these animal findings still do not answer the human question, which is where the evidence gets thinner again.
| Feature | Study 3: Rodent Lifespan | Study 4: Tumors & Oxidative Stress | Study 5: Genomic Stability |
|---|---|---|---|
| Model | Female SHR/CBA mice and rats; treatment often started around 3 months of age | Female mice, including CBA and HER-2/neu transgenic models | Aged rodents; bone marrow cells |
| Route & Schedule | Subcutaneous, microgram doses, short monthly courses | Intermittent courses over the lifespan | Subcutaneous, repeated courses |
| Main Outcome | Maximum lifespan +12.3%; last-decile survival +13.3%; other strains showed roughly 10–30% lifespan gains | Reduced spontaneous tumors, lower free-radical processes, mean survival +5.3%, maximum lifespan +10 months | Fewer chromosomal aberrations and better karyotypic stability |
| Mechanistic Signal | Inferred; no direct telomere measurement | Indirect; reduced oxidative DNA damage and tumor burden | Genomic-stability signal present; telomere mechanism unproven |
| Translational Caveats | Single-lab dominance; effects vary by sex, strain, and environment; unclear human dose scaling | Telomere mechanism is indirect; pathways incompletely mapped | Direct in vivo telomere data are sparse and methodologically inconsistent |
The animal data look promising, but they are not enough on their own. The human studies are what show whether these signals matter in clinical use.
Two human studies on mortality, telomere length, and functional aging markers
In humans, the story gets narrower. Instead of clean mechanistic signals, you mostly see older, non-randomized cohorts and small marker studies. The human evidence is thin, comes mostly from one research group, and has clear design problems.
Study 6: Long-term coronary patient follow-up study
Design and population: This was a non-randomized cohort, not a blinded RCT. Elderly patients with accelerated cardiovascular decline received repeated short epithalamin courses plus standard care, while controls received standard care alone. Follow-up lasted 12 to 15 years.
Main findings: The authors reported that epithalamin lowered all-cause mortality by about 28% and cardiovascular mortality by about 50%. They also reported similar drops in cardiovascular failure and respiratory disease. The same cohort was said to show better endurance, a more normal melatonin rhythm, and improved carbohydrate and lipid metabolism.
Caveats: There were no telomere endpoints, so these mortality results do not show a telomere effect. Key trial details, like allocation concealment, blinding, and protocol registration, are poorly described. That leaves plenty of room for selection bias. On top of that, no independent group has reproduced these mortality results in the 20-plus years since publication.
Study 7 shifts the focus from mortality to telomere-adjacent markers.
Study 7: Older-adult telomere and circadian marker studies
Where Study 6 follows mortality, Study 7 looks at telomere and circadian markers in smaller cohorts of older adults. These human data come from smaller mechanistic studies and small case series, often in people with sleep or circadian complaints or cardiovascular risk factors. In a 6-year cohort of 266 adults age 60 and older, epithalamin alone reduced mortality 1.6- to 1.8-fold versus controls, and annual epithalamin-plus-thymalin courses were linked to a 4.1-fold reduction.
Main findings: Related small studies reported higher nighttime melatonin levels, clearer day-night melatonin patterns, and self-reported sleep gains. Some small case series also described leukocyte telomere increases of 0.1 to 0.2 kb, along with better biological age scores.
Caveats: The telomere findings are the weakest part of the human evidence. No large human trial has used leukocyte telomere length as a prespecified primary endpoint for Epitalon or epithalamin. qPCR telomere assays can vary a lot, and a single follow-up reading can give a shaky picture of true biological change. There’s another big problem: these protocols often bundled Epitalon with other peptides and lifestyle changes, so you can’t tell what caused what. And all of this comes from the same research group, with no independent verification.
| Feature | Study 6: Coronary Patients | Study 7: Older Adults / Circadian Cohort |
|---|---|---|
| Population | Elderly patients with coronary artery disease | Adults 60+; smaller circadian/telomere sub-cohorts |
| Intervention | Repeated epithalamin courses vs. standard care | Epithalamin ± thymalin; smaller telomere protocols |
| Main outcomes | Mortality; endurance; circadian/metabolic markers | Mortality; melatonin rhythm; sleep; LTL |
| Telomere outcome | None | Small LTL increases in some case series |
| Key bias risks | Non-randomized, unclear blinding, no independent replication | Small N, heterogeneous protocols, bundled interventions |
Clinical bottom line for U.S. prescribers
After looking at each study, the practical question is simple: does any of this support routine prescribing? At this point, no. The pattern stays the same across the literature: strong mechanistic data, mixed animal results, and weak human evidence. That makes Epitalon a candidate for more study, not for routine anti-aging use.
The main clinical worry comes straight from the mechanism. Telomerase activation can support tumor biology, and that cancer risk is biologically grounded, not speculative. On top of that, there is no FDA-approved product, no standardized pharmacokinetic profile, and no human dose-response data. Regulatory status is still unsettled, so check current Federal Register listings before prescribing.
For U.S. clinicians, the safest frame is to treat Epitalon as investigational. Avoid it in patients with active malignancy, a recent cancer history, or hereditary cancer syndromes, and do not use it in place of guideline-directed care. If it is used, document the rationale, get informed consent, and monitor routine labs plus age-appropriate cancer screening. Review our practical clinical guides for more on patient education and handling. PeptidePrescriber (peptideprescriber.com) offers evidence-based monographs, dosing protocol summaries, and regulatory references to support that process.
Key takeaways from the seven-study roundup
For a quick scan, the table below shows what each study adds and how much weight it should carry in practice.
| Study type | Model / population | Primary outcome(s) | Evidence strength | Clinical relevance |
|---|---|---|---|---|
| Khavinson 2003 fibroblast study | Human fetal fibroblasts (in vitro) | ↑ hTERT, ↑ telomerase, telomere elongation | Strong lab evidence | Mechanistic only |
| Brunel University replication (2025) | Normal human cell lines | Telomerase activation, telomere lengthening | Strong, independent lab | Mechanistic only |
| Rodent lifespan studies | Aged rats and transgenic mice | Lifespan shifts, ↓ tumor incidence | Moderate (model-dependent) | Hypothesis-generating |
| Animal oxidative stress / genomic stability | Various rodent models | Oxidative markers, DNA stability | Moderate | Hypothesis-generating |
| Coronary patient follow-up | Human coronary cohort | Mortality, cardiovascular outcomes | Weak–moderate (observational) | Clinically oriented, indirect |
| Circadian / aging marker studies | Older adults; peptide mixtures | Sleep, melatonin, functional markers | Weak–moderate | Surrogate endpoints only |
| Human telomere/function markers | Small human cohorts | Leukocyte telomere length, functional aging markers | Weak (small, non-randomized) | Not yet clinically actionable |
Until large randomized human trials exist, Epitalon should remain investigational.
FAQs
Is Epitalon legal to prescribe in the U.S.?
No. Epitalon is not appropriate for routine clinical prescribing in the United States.
As of April 2026, the FDA placed it on a removal notice list. In plain terms, that move effectively shut down legal compounding channels for human use.
Prescribers should confirm the FDA’s current position through the Federal Register, since getting it outside authorized channels carries serious regulatory and safety risks.
Could telomerase activation from Epitalon increase cancer risk?
The search results provided don’t answer the key question: whether telomerase activation from Epitalon may increase cancer risk.
For evidence-based peptide safety and therapy monographs, see PeptidePrescriber.
Why don’t human studies prove Epitalon works yet?
Human studies on Epitalon are still inconclusive. The evidence is preliminary, and most of it comes from animal research, not people. Human data is still very limited.
For a treatment to have strong clinical backing, researchers usually need multiple well-designed randomized controlled trials that point in the same direction, or one large study with more than 500 participants. That bar matters. Small studies with around 20 people are much more likely to produce false positives, which means Epitalon’s efficacy still hasn’t been confirmed.