
If you want the short answer: most peptides in this area do not have strong human sleep data. In U.S. practice, the clearest sleep results still come from FDA-approved orexin drugs and melatonin-pathway treatments. For brain recovery, Cerebrolysin has the most human trial data, but it is still investigational in the United States.
Here’s the plain-English takeaway:
- Best-supported for sleep: orexin antagonists and melatonin-based drugs
- Low-risk add-on: glycine or collagen peptides, with small gains in sleep quality and next-day alertness
- Weak support: DSIP, due to old studies, mixed results, short half-life, and FDA safety concerns
- Best-supported for neuro recovery: Cerebrolysin after TBI or stroke, though U.S. approval is still absent
- Mostly early-stage: Semax, GHK-Cu, and BPC-157
A few numbers stand out:
- 19 RCTs, 1,683 people: melatonin cut sleep-onset latency by 7.06 minutes and added 8.25 minutes of total sleep time
- Meta-analysis, 7 DSIP trials, 94 people: effect size for sleep-onset latency was d=0.12, which was not different from zero
- Collagen peptide study, 63 people: 5 g nightly led to small gains in sleep quality and less daytime sleepiness
- Glycine before bed: 3 g cut sleep-onset latency by about 10 minutes and improved next-day alertness
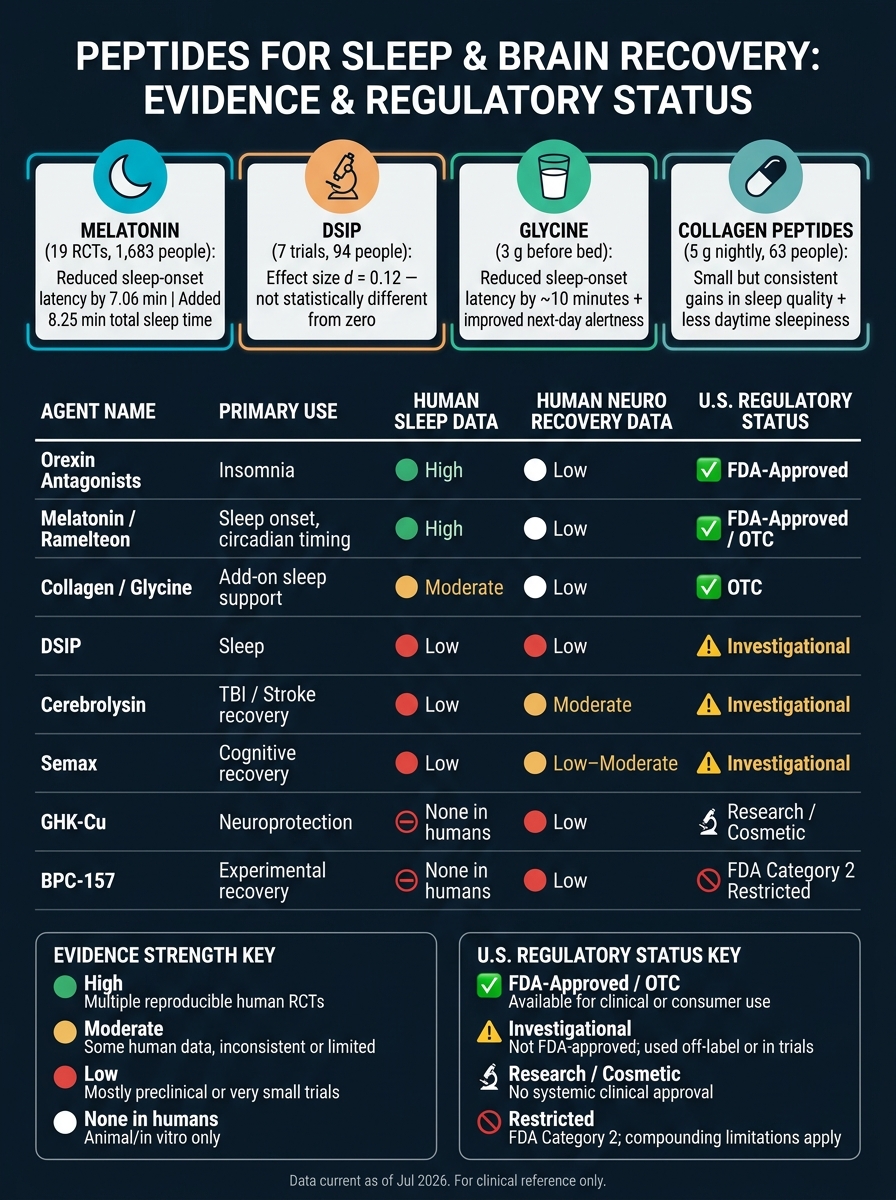
Peptides for Sleep & Brain Recovery: Evidence & Regulatory Status at a Glance
How Pinealon Might Improve Sleep & Cognitive Function | Dr. Abud Bakri & Dr. Andrew Huberman
sbb-itb-7164bd9
Quick Comparison
| Agent | Main Use | Human Sleep Data | Human Neuro Recovery Data | U.S. Status |
|---|---|---|---|---|
| Orexin antagonists | Insomnia | High | Low | FDA-approved |
| Melatonin / ramelteon | Sleep onset, circadian timing | High | Low | OTC / FDA-approved |
| Collagen / glycine | Add-on sleep support | Moderate | Low | OTC |
| DSIP | Sleep | Low | Low | Investigational |
| Cerebrolysin | TBI / stroke recovery | Low | Moderate | Investigational |
| Semax | Cognitive recovery | Low | Low–moderate | Investigational |
| GHK-Cu | Neuroprotection signals | None in humans | Low | Research / cosmetic use |
| BPC-157 | Experimental recovery claims | None in humans | Low | Restricted compounding status |
If I were summarizing the article in one line, I’d say this: sleep care has a few options with human proof, but most “recovery peptides” still sit far behind standard U.S. treatment pathways.
Peptides with the strongest clinical data for sleep outcomes
Building on the evidence tiers above, the agents here have the strongest human sleep data. The next three subsections split the best-supported sleep agents from weaker or add-on options.
DSIP: human insomnia data and conflicting findings
Delta sleep-inducing peptide (DSIP) was one of the first peptides studied for sleep. Early trials from the 1970s and 1980s reported gains in slow-wave sleep and shorter sleep-onset latency. In one small trial in people with chronic insomnia, DSIP increased total sleep time by 59% within 130 minutes of dosing compared with placebo. That result stands out, but it has not been repeated.
The problem is consistency. Early studies pointed to a possible effect, but later polysomnography work did not back it up. A 1988 meta-analysis of seven controlled DSIP trials (n=94) found a weighted mean effect size of d=0.12 for reducing sleep-onset latency, which was not different from zero in statistical terms. Its pharmacokinetics also make a strong central nervous system effect harder to argue for: DSIP has a plasma half-life of less than 15 minutes and poor blood-brain barrier penetration. The FDA has also flagged compounded DSIP formulations for potential immunogenicity risk, which adds another layer of concern. Put simply, DSIP has weak clinical support.
By contrast, melatonin-based agents show steadier human results.
Melatonin receptor agonists and analogs
Across 19 RCTs (n=1,683), melatonin reduced sleep-onset latency by 7.06 minutes and increased total sleep time by 8.25 minutes. Those gains are modest, but they show up again and again. Its effect on sleep architecture is minimal.
Next-generation melatonin signaling agents target MT1 and MT2 receptors. Ramelteon is the main example. These drugs are FDA-approved and used in U.S. practice mainly for circadian rhythm disorders and trouble falling asleep. They work through a more targeted pathway than OTC melatonin.
That matters because OTC melatonin has a major quality issue. In one analysis, products showed dose variability from -83% to +478% of the labeled amount. That's not a small miss. It's the kind of gap that can turn a simple sleep aid into a guessing game. Third-party testing matters here.
Beyond circadian signaling, the strongest insomnia trial data sit with orexin blockade.
Orexin antagonists and bedtime collagen or glycine peptides
The clearest signal in current sleep pharmacology comes from dual orexin receptor antagonists, or DORAs. Drugs such as suvorexant and lemborexant block the brain's orexin system, which helps drive wakefulness. Both are FDA-approved for insomnia. Their results have been reproduced across human trials.
At the milder end, glycine-rich collagen peptides may help as an add-on. Collagen is about 35% glycine by mass, and glycine acts as an inhibitory neurotransmitter. A 2019 study of 63 participants found that 5 g of nightly collagen peptides led to modest gains in subjective sleep quality and less daytime sleepiness. In a separate line of research, 3 g of glycine taken before bed reduced sleep-onset latency by about 10 minutes and improved next-day alertness and cognitive performance. The effect sizes are small, but the safety profile is very high and the mechanism is well described, which makes this a practical low-risk option for clinicians who want add-on support.
The table below compresses the clinical takeaways for quick reference.
| Agent | Key Sleep Endpoint | Evidence Consistency | U.S. Status |
|---|---|---|---|
| Orexin Antagonists | Sleep induction and maintenance | High - reproducible human trials | FDA-approved (Rx) |
| Melatonin signaling agents | Sleep onset, circadian timing | High for timing; minimal for architecture | OTC (melatonin); Rx (ramelteon) |
| Collagen / Glycine | Sleep-onset latency, subjective quality | Moderate - modest, consistent gains | OTC supplement |
| DSIP | Sleep-onset latency, slow-wave sleep | Low - not replicated in modern RCTs | Not approved; immunogenicity risk |
Peptides studied for cognitive recovery and neuroprotection
Sleep is only part of the story. The bigger clinical question is whether peptides help with next-day thinking after sleep loss or support recovery after CNS injury, such as TBI or stroke. That’s where this group of compounds comes in.
Some of the data come from human randomized trials. Some of it comes almost entirely from animal work. So the gap between agents is pretty wide.
Cerebrolysin: controlled data on recovery after brain injury and stroke
Cerebrolysin is a porcine peptide preparation with proposed neurotrophic activity and CNS penetration. Among the peptides in this group, it has the strongest clinical data.
Controlled studies suggest benefit after TBI, including faster cognitive symptom resolution in mild TBI and functional improvement in moderate-to-severe TBI.
The stroke picture is less clear. One trial favored motor recovery, but a 2023 Cochrane review found no mortality benefit and noted possible harm. That tension matters. If you’re reading the Cerebrolysin literature, you can’t just look at the positive trials and call it a day.
Cerebrolysin is approved in over 44 countries, but in the United States it remains investigational and is not FDA-approved.
The next agents have much weaker human data and lean mostly on preclinical signals.
GHK-Cu and Semax: signals for neuroprotection and cognitive resilience
GHK-Cu and Semax sit in a very different evidence tier.
GHK-Cu has only preclinical support, including a mouse study that showed protection against sleep-deprivation-related learning impairment. That’s interesting, but it’s still animal data.
Semax has limited human evidence and is supported mainly by regional clinical and animal data. In plain English: there are signals, but not the kind of clinical base that lets you make strong claims.
Neither agent has FDA approval. Clinicians can use dosing protocols to navigate these investigational compounds.
BPC-157 and other preclinical cognitive peptides
BPC-157 is still a preclinical compound, with no established clinical utility for cognitive recovery.
| Peptide | Evidence Level | Primary Mechanism |
|---|---|---|
| Cerebrolysin | High (human RCTs) | Multimodal neurotrophic mimicry (BDNF, NGF, GDNF, CNTF) |
| Semax | Moderate | BDNF upregulation; cognitive rehabilitation |
| GHK-Cu | Low/Emerging | Antioxidant; reduces MCP-1 and nitrotyrosine |
| BPC-157 | Low | CNS repair and neurovascular recovery signals |
Comparing evidence, safety, and U.S. regulatory status
Evidence strength, safety signals, and approved versus investigational use
Once you look at sleep agents and neurorecovery compounds side by side, the practical issue becomes pretty simple: which ones actually have human data, a safety profile clinicians can work with, and clear relevance in the United States?
The biggest split is approved treatment vs. investigational use. Orexin antagonists and melatonin receptor agonists sit at the top for U.S.-relevant insomnia care. They have the strongest data and the clearest safety picture. That said, they’re not risk-free. Orexin antagonists can lead to daytime somnolence and complex sleep behaviors. Melatonin receptor agonists are more often linked to dizziness or fatigue.
The other agents are less convincing, or at least less useful in day-to-day clinical care. DSIP falls into that bucket. Its clinical value is weak because the signal is old, small, and hasn’t been replicated. The early signal came from IV studies, and there’s still no validated receptor or mechanism.
On the neurorecovery side, Semax is still investigational in U.S. practice. GHK-Cu is backed mostly by preclinical neuroprotection signals. BPC-157 is listed by FDA as a Category 2 bulk substance, which limits compounding use. For U.S. clinicians, that makes routine use hard to justify.
Cerebrolysin stands out as the strongest neurorecovery candidate in this group. It has human trial data from international stroke and TBI studies. Even so, it remains investigational and is not approved by the FDA in the United States.
Summary table: peptide comparison for clinical reference
The table below compresses the clinical hierarchy into a quick bedside reference.
| Peptide / Class | Evidence Strength | Sleep Use | Neurorecovery Use | Key Safety Issue | U.S. regulatory landscape |
|---|---|---|---|---|---|
| Orexin Antagonists | High | Improves sleep onset and maintenance | Not primary indication | Daytime somnolence; complex sleep behaviors | FDA-Approved |
| Melatonin Agonists | High | Circadian rhythm regulation; sleep onset | Not primary indication | Dizziness, fatigue | FDA-Approved / OTC |
| DSIP | Low–Moderate | Mixed; signal not replicated in modern RCTs | Not established | Short half-life; IV data only | Investigational |
| Cerebrolysin | Moderate | Not studied | Stroke and TBI recovery data | Porcine-derived; safety data from international trials | Investigational |
| Semax | Low | Limited | Cognitive and neuroprotection signals | Limited independent Western replication | Investigational |
| GHK-Cu | Low | None in humans | Neuroprotection signals | Topical safety better established than systemic | Research / Cosmetic use |
| BPC-157 | Low | None in humans | No established clinical utility | No direct human safety data | FDA Category 2 (Restricted) |
Conclusion: Key takeaways for sleep and brain recovery care using peptides
The main takeaway from this research is simple: the quality of evidence varies a lot across these peptides.
For sleep, orexin antagonists have the strongest human data. Melatonin also stands on firmer ground, with multiple randomized trials showing modest gains in sleep latency and sleep quality. DSIP has shown a signal in older research, but the data is dated, small, and inconsistent. The same issue shows up in cognitive recovery, where the human evidence base is even thinner.
For neurologic recovery, Cerebrolysin has the strongest human data. The other agents are still investigational or remain in the preclinical stage, and movement into clinical use has been limited.
That narrows routine U.S. use to agents with clearer approval status and safer prescribing paths. As of Jul 2026, DSIP, BPC-157, and Epitalon remain under FDA review for 503A bulk drug substance status, and DSIP is in Category 2 because of safety and effectiveness concerns.
In practice, patient selection, objective endpoints, and finite treatment cycles matter more than peptide choice alone.
For protocol support, PeptidePrescriber provides evidence-based monographs, dosing tools, and regulatory references for clinicians.
FAQs
Which options have the best human sleep data?
DSIP has the strongest human research base here, at least when you look specifically at sleep architecture. That said, there’s a catch: much of that evidence comes from older studies, and the study design wasn’t as tight as what we’d expect today. Those earlier papers reported shorter sleep onset latency and more deep sleep, but modern large-scale, placebo-controlled trials still haven’t shown up.
GHS options, such as ghrelin, GHRH analogs, and Ipamorelin, are also used for sleep support, though in a more indirect way. The idea is pretty simple: they may help amplify natural growth hormone pulses that tend to occur during slow-wave sleep.
Are any of these peptides FDA-approved in the U.S.?
No. Peptides often mentioned for sleep and brain recovery, including DSIP and epithalon, are not FDA-approved in the U.S. for insomnia or other sleep disorders.
A few, like sermorelin, had FDA approval in the past for other uses. But that’s a different lane. They were not approved for sleep enhancement, and they are not approved for that use now.
In the U.S., these compounds are viewed as investigational. Historically, they’ve also been used through compounding pharmacies while remaining under FDA review.
How strong is the evidence for brain recovery peptides?
Evidence is not evenly spread across these compounds.
Cerebrolysin has the strongest clinical backing. It’s been studied in multiple randomized, double-blind, placebo-controlled trials, including the CAPTAIN program. Meta-analyses also report statistically significant gains in neurological and functional outcomes in traumatic brain injury and dementia.
Other peptides don’t have the same level of support. Sleep-related peptides like DSIP are backed mostly by smaller, older studies, and many of those studies don’t meet current standards for study design and quality.