
If you're exploring growth hormone-releasing peptides, CJC-1295 and Ipamorelin are two of the most commonly used options. Here's the key takeaway:
- CJC-1295 (No-DAC) stimulates the pituitary gland to prepare for growth hormone (GH) release, mimicking natural rhythms. It's typically dosed daily for short bursts of GH production.
- Ipamorelin triggers immediate GH release without affecting cortisol or prolactin levels, making it a selective and safe option for most users.
- CJC-1295 with DAC offers long-lasting GH stimulation with fewer injections but may interfere with natural GH pulsatility.
For best results, combining CJC-1295 (No-DAC) and Ipamorelin creates a synergistic effect, amplifying GH release 3–5 times more than either peptide alone. This combination is ideal for improving recovery, sleep, body composition, and overall well-being.
Quick Comparison
| Feature | CJC-1295 (No-DAC) | Ipamorelin | CJC-1295 (With DAC) |
|---|---|---|---|
| Action | Prepares GH release | Triggers GH pulse | Sustained GH release |
| Half-Life | ~30 minutes | ~2 hours | 6–8 days |
| Dosing | 1–3× daily | 1–3× daily | 1–2× weekly |
| Best For | Natural GH rhythms | Sharp GH spikes | Convenience-focused |
| Side Effects | Minimal | Minimal | Water retention risk |
If you're new to peptides, starting with a conservative dose of the CJC-1295 (No-DAC) + Ipamorelin combo is often recommended. Always consult a healthcare provider to tailor the protocol to your goals and monitor IGF-1 levels for safety.
CJC-1295 vs Ipamorelin: Full Peptide Protocol Comparison
Mechanistic and Pharmacokinetic Comparison
Receptor Targets and Combined Mechanisms
To tailor treatments effectively, it’s important to grasp how CJC-1295 and Ipamorelin target receptors and interact within the body.
CJC-1295 works by binding to the GHRH receptor (GHRH-R) on pituitary somatotroph cells. This interaction activates the cAMP/PKA signaling pathway, which promotes GH gene transcription and prepares the pituitary gland for growth hormone (GH) release. On the other hand, Ipamorelin targets the ghrelin receptor (GHS-R1a) and activates the PLC/IP3/Ca²⁺ pathway. This not only triggers GH release but also inhibits somatostatin, GH's natural suppressor. Similar mechanisms are observed with other GHRH analogs like Sermorelin.
"The GHRH pathway sets the amplitude of the GH pulse, while the ghrelin pathway potentiates the pituitary's sensitivity to that signal." - Dr. Julian Douwes
When combined, these two peptides amplify each other's effects, creating a GH pulse that is 3 to 5 times larger than what either peptide could produce alone. Their complementary mechanisms make this combination particularly effective. Next, let’s look at how their half-lives shape dosing strategies.
Half-Life and Dosing Patterns
CJC-1295 without DAC (also known as Mod GRF 1-29) has a short half-life of about 30 minutes, making it suitable for pulsatile dosing that mirrors the body's natural GH cycles. Ipamorelin, with a longer half-life of approximately 2 hours, generates a distinct and sharp GH pulse.
The DAC version of CJC-1295, which binds to serum albumin, extends its half-life significantly to 6–8 days. While this allows for once- or twice-weekly dosing, the sustained "GH bleed" it produces can lead to receptor downregulation. For this reason, it is less commonly used in combination protocols that aim to preserve natural GH pulsatility.
For those prioritizing a dosing method that aligns with the body's natural rhythms, pairing CJC-1295 without DAC with Ipamorelin is often the go-to choice. This approach is discussed further in the dosing protocols section.
Pharmacological Differences: Comparison Table
Here’s a quick breakdown of the key differences between these peptides:
| Property | CJC-1295 (No DAC) | Ipamorelin | CJC-1295 (With DAC) |
|---|---|---|---|
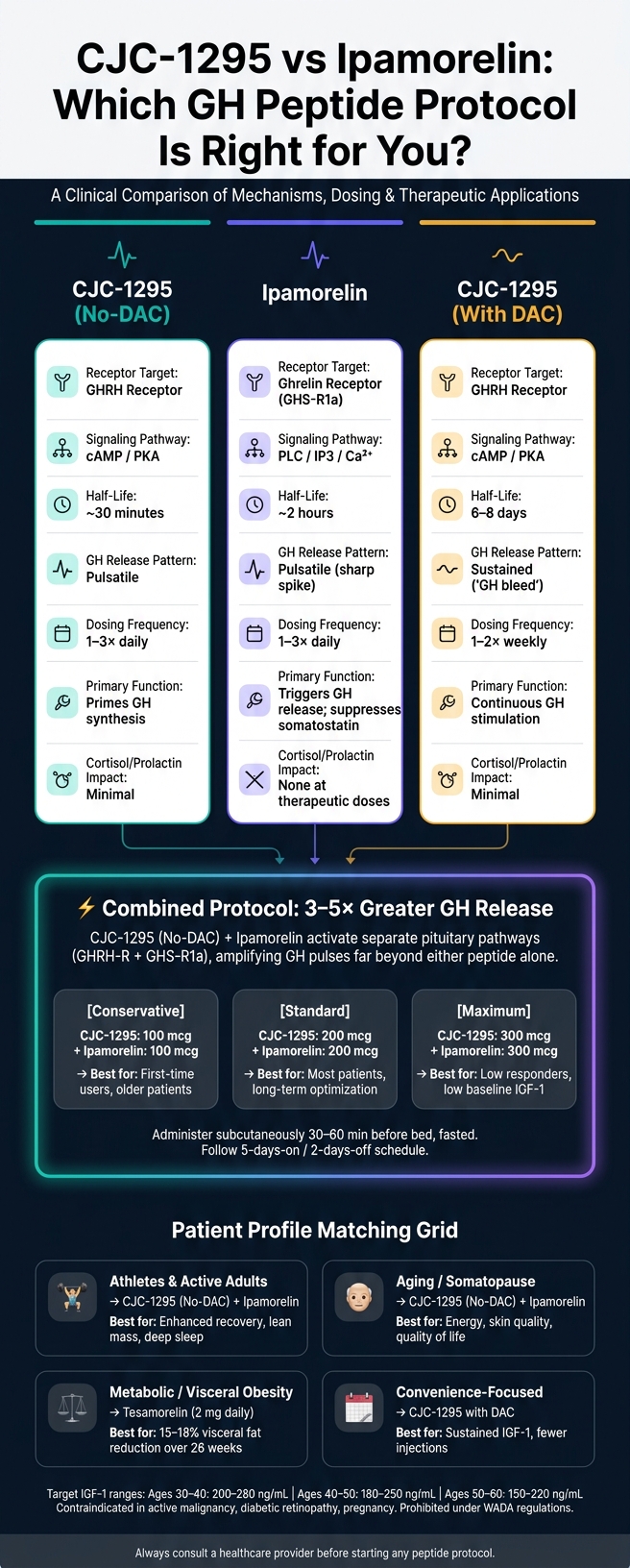
| Receptor Target | GHRH Receptor | Ghrelin Receptor (GHS-R1a) | GHRH Receptor |
| Signaling Pathway | cAMP / PKA | PLC / IP3 / Ca²⁺ | cAMP / PKA |
| Half-Life | ~30 minutes | ~2 hours | 6–8 days |
| GH Release Pattern | Pulsatile | Pulsatile (sharp spike) | Sustained ("GH bleed") |
| Dosing Frequency | 1–3× daily | 1–3× daily | 1–2× weekly |
| Primary Function | Primes GH synthesis | Triggers GH release; suppresses somatostatin | Continuous GH stimulation |
| Cortisol/Prolactin Impact | Minimal | None at therapeutic doses | Minimal |
sbb-itb-7164bd9
CJC-1295, Ipamorelin, Tesamorelin & Sermorelin: Deep Dive on the Best GH Peptides
Dosing Protocols and Administration
Let's dive into the dosing protocols and practical tips for administering CJC-1295 and Ipamorelin, building on their pharmacokinetic differences.
Monotherapy Protocols for CJC-1295 and Ipamorelin
Each peptide has its own dosing structure, which varies depending on whether you're using CJC-1295 with or without DAC.
- CJC-1295 without DAC (Mod GRF 1-29): Dosage ranges from 100–300 mcg, administered 5–6 nights per week. It should be taken 30–60 minutes before bed on an empty stomach.
- CJC-1295 with DAC: Due to its longer half-life, this form is dosed at 1–2 mg once or twice per week, making timing less critical.
- Ipamorelin monotherapy: This mirrors the No-DAC protocol, with 100–300 mcg taken 5–7 nights per week before sleep.
Timing is crucial. Richard Lemke, Founder of The Peptide Toolkit, emphasizes:
"The fasted-state requirement is non-negotiable. Insulin (post-meal) and elevated free fatty acids (post-fatty-meal) both blunt GH release."
Patients should fast for 2–3 hours before injection and wait 20–30 minutes afterward for the best results.
While monotherapy focuses on individual peptides, combining them can amplify growth hormone (GH) responses.
Combination Protocols: CJC-1295 and Ipamorelin
The combination of CJC-1295 No-DAC and Ipamorelin is widely used for GH optimization. Administered together at bedtime, they work on separate receptor pathways - GHRH-R and GHS-R1a - to create a GH pulse 3–5 times larger than using either peptide alone.
Dosing is adjusted based on patient needs and IGF-1 levels:
| Tier | CJC-1295 (No-DAC) | Ipamorelin | Best For |
|---|---|---|---|
| Conservative | 100 mcg | 100 mcg | First-time users, older patients |
| Standard | 200 mcg | 200 mcg | Most patients, long-term optimization |
| Maximum | 300 mcg | 300 mcg | Low responders or patients with low baseline IGF-1 |
New patients typically start on the conservative tier for two weeks, with adjustments made as needed. Since pituitary saturation occurs at around 100 mcg per injection, doses above 200–300 mcg may offer diminishing returns and increase the risk of side effects like water retention. Most protocols follow a 5-days-on, 2-days-off schedule to maintain pituitary sensitivity and avoid receptor desensitization.
"CJC-1295/Ipamorelin is typically dosed at 100–300 mcg of each peptide subcutaneously before bed, 5–6 nights per week... the combination is the workhorse protocol." - Dr. Julian Douwes, M.D.
Administration Tips for Clinicians
Subcutaneous injection into abdominal fat is the preferred method for both peptides. Use a 29–31 gauge insulin syringe and inject at a 45–90 degree angle, about 2 inches from the navel. Other viable sites include the outer thigh and upper arm. To prevent irritation or tissue changes, rotate injection sites daily.
When reconstituting lyophilized peptides, direct the bacteriostatic water along the glass wall and gently swirl to avoid damaging the peptide structure. Store reconstituted peptides in the refrigerator at 36–46°F (2–8°C), away from light, and use within 21–30 days.
The monthly cost for a standard combination protocol typically ranges from $200–$400 for compounded blends, with an additional $20–$30/month for supplies like syringes, alcohol wipes, and bacteriostatic water. Following these guidelines helps ensure safe and effective administration while setting the stage for monitoring and managing any potential side effects.
Therapeutic Applications by Patient Profile
Matching peptide protocols to a patient's clinical goals is essential, as pharmacokinetic differences directly impact therapeutic applications.
Body Composition and Metabolic Effects
The combination of CJC-1295 and Ipamorelin is often used to improve body composition. CJC-1295 provides a sustained increase in IGF-1, aiding in lean muscle retention and protein synthesis. Meanwhile, Ipamorelin delivers acute growth hormone pulses that promote fat breakdown, particularly targeting visceral fat. Patients typically see IGF-1 levels rise by 50–150 ng/mL within 4–8 weeks.
For individuals dealing with significant visceral fat or metabolic syndrome, Tesamorelin has shown a 15–18% reduction in visceral fat over 26 weeks. However, it’s important to manage expectations, as results with Tesamorelin differ from those seen with CJC-1295 and Ipamorelin.
"The CJC-1295/Ipamorelin combination is the workhorse protocol... you stimulate your own pituitary gland to release growth hormone in a pattern that approximates physiological secretion." - Dr. Julian Douwes, M.D.
In addition to metabolic benefits, these peptides contribute to better sleep and improved recovery.
Sleep, Recovery, and Quality of Life
A large portion of growth hormone (50–70%) is secreted during the first two hours of deep sleep. Administering CJC-1295 and Ipamorelin 30–60 minutes before bedtime supports this natural hormone surge, enhancing tissue repair, collagen production, and muscle protein synthesis.
Ipamorelin’s targeted action avoids raising cortisol or prolactin levels, which helps maintain healthy sleep patterns and metabolic stability.
"The combination essentially mimics the way the hypothalamus naturally orchestrates peak GH release during deep sleep: a GHRH surge... coincides with falling somatostatin and rising ghrelin." - Dr. Priyali Singh, M.D.
For patients focused on sleep and recovery, CJC-1295 without DAC is preferred, as it preserves the natural pulsatility of growth hormone release. In contrast, the DAC version creates a continuous elevation, which might interfere with the body’s natural rhythms.
Patient Selection and Protocol Matching
Choosing the right protocol depends on the patient’s goals, age, and tolerance for injections. The table below outlines common profiles and their recommended approaches:
| Patient Profile | Recommended Protocol | Primary Benefit |
|---|---|---|
| Athletes & Active Adults | CJC-1295 (No-DAC) + Ipamorelin | Enhanced recovery, lean mass retention, deep sleep |
| Aging / Somatopause | CJC-1295 (No-DAC) + Ipamorelin | Improved energy, skin quality, and quality of life |
| Metabolic / Visceral Obesity | Tesamorelin (Daily 2 mg) | Targeted visceral fat reduction, improved lipids |
| Convenience-Focused Patients | CJC-1295 with DAC | Sustained IGF-1 elevation with less frequent dosing |
Clinicians should aim for IGF-1 levels that align with age-appropriate ranges: 200–280 ng/mL for ages 30–40, 180–250 ng/mL for ages 40–50, and 150–220 ng/mL for ages 50–60. As Dr. Priyali Singh, M.D., explains, the objective is to restore IGF-1 to functional levels appropriate for the patient’s age, rather than exceeding natural limits.
Absolute contraindications include active malignancy, diabetic retinopathy, and pregnancy. Additionally, both peptides are prohibited for competitive athletes under WADA regulations.
Adverse Effects, Monitoring, and Risk Mitigation
Potential Adverse Effects
While both peptides are generally well-tolerated, it’s important for clinicians to set clear expectations with patients from the outset. The most common side effects include mild injection-site redness, temporary flushing, and transient water retention. These effects typically resolve on their own within one to two weeks.
Ipamorelin stands out for its selectivity compared to older secretagogues like GHRP-2 or GHRP-6. At therapeutic doses, it does not significantly increase cortisol, ACTH, or prolactin levels. As Dr. Julian Douwes, M.D., explains: "Ipamorelin stimulates GH release without significantly increasing cortisol, prolactin, or ACTH. This selectivity is clinically important."
CJC-1295 with DAC, however, has a different risk profile. With its 6–8 day half-life, it promotes sustained GH release rather than the natural pulsatile pattern, which can lead to more pronounced water retention and, in some cases, numbness or tingling in extremities. On the other hand, the no-DAC version preserves the natural pulsatility of GH.
These side effects highlight the need for careful monitoring and dose adjustments to ensure safe and effective treatment.
| Side Effect | Frequency | Management |
|---|---|---|
| Water retention/Edema | Common | Lower the dose; reduce dietary sodium; typically resolves within 1–2 weeks |
| Numbness/Tingling | Common at high doses | Reduce dose; reflects elevated IGF-1 |
| Flushing/Warmth | Common | Self-limiting; usually lasts 1–3 minutes post-injection |
| Injection-site redness | Occasional | Rotate injection sites; ensure proper subcutaneous technique |
| Increased hunger | Uncommon | Mild and far less noticeable compared to GHRP-6 |
Monitoring Recommendations
To manage therapy effectively, clinicians should follow a structured monitoring protocol. Accurate and timely testing ensures that treatment remains safe and tailored to each patient’s needs.
Before starting therapy, baseline labs should include IGF-1, fasting glucose, insulin (HOMA-IR), HbA1c, a complete metabolic panel (CMP), and a lipid panel. For men over 40, a PSA test is also recommended due to IGF-1's potential mitogenic effects.
The first follow-up IGF-1 test should occur 4–6 weeks after starting treatment to assess the patient’s response and make any necessary dose adjustments. For stable patients, comprehensive testing every 3–6 months is sufficient. Clinicians should be cautious of IGF-1 levels consistently exceeding 300 ng/mL, as this may increase cancer risk. Dr. Julian Douwes, M.D., advises: "IGF-1 levels consistently above 300 ng/mL warrant dose reduction. Chronically elevated IGF-1 is associated with increased cancer risk in epidemiological studies."
| Monitoring Timepoint | Recommended Tests |
|---|---|
| Baseline | IGF-1, fasting glucose, insulin, HbA1c, CMP, lipid panel, PSA (if applicable) |
| 4–6 Weeks | IGF-1 (to confirm response and adjust dose) |
| 8–12 Weeks | IGF-1, fasting glucose, insulin, HbA1c |
| 6 Months | Full panel (CMP, lipid panel, IGF-1) and body composition assessment |
Protocol Adjustments and Discontinuation Criteria
To minimize risks, dose adjustments should be made promptly if patients experience symptoms like numbness, tingling, or persistent edema - indicators that IGF-1 levels may be too high. In such cases, clinicians should reduce the dose incrementally and recheck labs after approximately four weeks.
A cycling protocol of 12 weeks on and 4 weeks off helps maintain pituitary receptor sensitivity and allows for a baseline reassessment without exogenous stimulation. Additionally, some clinicians adopt a 5-days-on, 2-days-off weekly schedule to further prevent receptor downregulation.
Therapy should be discontinued immediately if the patient develops active malignancy, proliferative diabetic retinopathy, uncontrolled hyperglycemia, or a new pituitary tumor. Pregnancy and breastfeeding are also absolute contraindications. For patients with cardiovascular risk factors, the historical cardiac safety concerns noted during a Phase II trial of CJC-1295 DAC - despite the myocardial infarction being deemed unrelated - should be carefully considered when evaluating the DAC formulation.
Conclusion and Key Takeaways
Choosing between CJC-1295 and Ipamorelin isn’t a one-size-fits-all decision - it’s all about individual needs. Ipamorelin stands out as a more selective option, providing growth hormone (GH) pulses without affecting cortisol, prolactin, or ACTH levels. On the other hand, CJC-1295 with DAC offers the convenience of fewer injections by keeping IGF-1 levels elevated for 9–11 days, though it does so at the cost of the natural GH pulsation.
Interestingly, combining these peptides can result in a powerful synergy. By activating separate pituitary pathways, the duo amplifies GH release far beyond what either can achieve alone. Dr. Cory Mellon, MD, likens their effect to a relay race:
"Think of CJC-1295 and Ipamorelin as relay partners. CJC-1295 is the long-distance runner... Ipamorelin is the sprinter... Together, they produce 3–5 times more growth hormone release than either peptide alone."
Here’s a quick comparison to guide your decision:
| Decision Factor | Choose Ipamorelin | Choose CJC-1295 (No-DAC) | Choose CJC-1295 (DAC) |
|---|---|---|---|
| Primary Goal | Clean, selective GH pulse | Enhanced pulsatile synergy | Stable IGF-1 with fewer injections |
| Dosing Preference | 1–3× daily | 1–3× daily | 1–2× weekly |
| Metabolic Sensitivity | High tolerability | Moderate | Requires closer monitoring |
| Adherence Advantage | Low concern | Low concern | Low concern (fewer injections) |
To maximize effectiveness, administer injections on an empty stomach, ideally 30–60 minutes before bedtime. Keep IGF-1 levels within an age-appropriate range and take breaks every 12–16 weeks to maintain receptor responsiveness. As Dr. Julian Douwes, MD, wisely points out:
"The peptide amplifies the signal your body is already producing. If that baseline signal is weak because the foundations are neglected, no secretagogue will compensate."
FAQs
How do I choose between CJC-1295 (No-DAC), Ipamorelin, and CJC-1295 (DAC)?
Your choice depends on what you're aiming for: a natural rhythm or steady, prolonged elevation of growth hormone levels.
- CJC-1295 (No-DAC) + Ipamorelin: This combination mimics the body's natural pulsatile release of growth hormone. Both peptides have short half-lives of about 30 minutes and require daily injections.
- CJC-1295 (DAC): Designed for sustained hormone elevation, this version has a much longer half-life of 6–8 days and is dosed weekly. It doesn't mimic the body's natural release patterns and is generally not combined with Ipamorelin.
What IGF-1 labs should I order, and how often?
Before beginning a CJC-1295 and Ipamorelin regimen, it’s important to measure your baseline IGF-1 (Insulin-like Growth Factor 1) levels. This helps track how your growth hormone activity responds to the treatment. Typically, IGF-1 levels increase by 50–150 ng/mL within 4 to 8 weeks. Most healthcare providers suggest follow-up lab tests between weeks 8 and 16 to evaluate progress. These results guide decisions on whether to adjust the dosage, continue therapy, or take a break with an off-cycle period.
Who should not use these peptides?
To determine whether these peptides are suitable for you, a comprehensive clinical evaluation is essential. Your healthcare provider will need to assess your medical history, lab results, current medications, symptoms, and any associated risk factors. It's important to note that these peptides may not be recommended for individuals with poorly managed metabolic markers, such as elevated blood sugar or IGF-1 levels. Always ensure treatment is guided by a qualified medical professional - never rely on non-clinical advice.