Peptide therapy is gaining traction among licensed prescribers due to its targeted approach to treating metabolic, endocrine, and regenerative conditions. This guide addresses key questions about patient selection, dosing, safety, and regulations.
Key Takeaways:
- What Are Peptides? Short amino acid chains that act as signaling molecules, interacting with specific receptors to produce precise biological effects.
- Why Use Peptides? They are highly specific, lower in immunogenicity, and often more affordable than larger biologics. Examples include insulin, semaglutide, and oxytocin.
- Who Qualifies? Patients with obesity, type 2 diabetes, cardiovascular risks, or specific conditions like HIV-associated lipodystrophy or hypoactive sexual desire disorder.
- Safety Considerations: Contraindications include conditions like Medullary Thyroid Carcinoma, gastroparesis, and pregnancy. Monitoring is essential to minimize risks.
- Regulations: Peptides must be sourced from FDA-compliant 503A or 503B facilities. Recent FDA changes restrict compounding of certain peptides like BPC-157 and CJC-1295.
Peptides offer a promising avenue for targeted therapies, but prescribers must stay informed about evolving regulations and ensure thorough documentation for safe practice.
Patient Selection and Treatment Planning
Which Patients Are Good Candidates for Peptide Therapy?
Peptide therapy is typically suited for adults dealing with metabolic challenges or obesity. Candidates often include those with type 2 diabetes, a BMI of 30 kg/m² or higher, or a BMI of 27 kg/m² or higher accompanied by at least one weight-related condition like hypertension or dyslipidemia. Patients with cardiovascular disease and excess weight may also benefit. For instance, semaglutide 2.4 mg has been shown to lower the risk of major adverse cardiovascular events by about 20% in non-diabetic individuals with obesity or overweight.
Beyond these metabolic conditions, specific peptides are approved for other purposes. Tesamorelin is used to reduce visceral fat in patients with HIV-associated lipodystrophy, while Bremelanotide (PT-141) is prescribed for premenopausal women experiencing hypoactive sexual desire disorder (HSDD). Additionally, semaglutide is an option for patients with noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH) and moderate-to-advanced liver fibrosis (stages F2–F3).
Here’s a quick overview of peptide types and their primary clinical applications:
| Peptide Type | Example Agents | Primary Clinical Indications |
|---|---|---|
| GLP-1 / Dual Agonists | Semaglutide, Tirzepatide | Type 2 Diabetes, Obesity, MASH, Cardiovascular Risk |
| GHRH / GHRPs | Tesamorelin, Sermorelin | HIV-associated Lipodystrophy, Pediatric GH Deficiency |
| Melanocortin Agonists | Bremelanotide (PT-141) | Hypoactive Sexual Desire Disorder (HSDD) |
| Amylin Analogs | Pramlintide | Adjunct to insulin in Type 1 and Type 2 Diabetes |
Understanding who qualifies for peptide therapy is only part of the equation. Knowing the contraindications is just as critical.
Contraindications and Cautions to Know
Certain conditions make peptide therapy unsuitable for some patients. GLP-1 or GIP/GLP-1 agonists, for example, should never be prescribed to individuals with a personal or family history of Medullary Thyroid Carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
"MOUNJARO is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)." - FDA Prescribing Information
Patients with severe gastroparesis or a history of pancreatitis are also excluded from using these therapies. Pregnancy is another key contraindication. Women planning to conceive must stop semaglutide at least two months in advance due to its long half-life and potential risks to the fetus. Female patients using oral contraceptives should switch to non-oral methods or add a barrier method for four weeks after dose escalation.
Growth hormone secretagogues and IGF-1 analogs come with their own risks, such as insulin resistance and possible tumor-promoting effects. For this reason, patients with active malignancies require extra caution when considering these options.
Setting Treatment Goals and Follow-Up Plans
Once a patient's eligibility and potential risks are determined, the next step is setting clear and measurable treatment goals. Start by conducting baseline lab tests, defining clinical objectives, and obtaining informed consent, especially for compounded or off-label use. Each prescription should directly address a specific clinical goal, such as achieving a target HbA1c level, reducing body weight by a certain percentage, or improving liver fibrosis staging.
"Every prescription is tied to a named clinical indication, not a vibe." - Joshua Hare, DO, Founder, Limitless Performance Medicine
For growth hormone peptides like Sermorelin and Ipamorelin, monitor IGF-1 levels every three months. Immune peptides, such as Thymosin Alpha-1, should be reassessed every 4–8 weeks. Tools like DEXA or InBody scans can help track changes in body composition.
Lastly, always stay up-to-date on the legal status of compounded peptides. For example, the FDA has reclassified several agents, including BPC-157, CJC-1295, and Ipamorelin, into Category 2 as of 2026, which prohibits their use in human compounding.
The Emerging Science and Clinical Application of Peptide Therapy
Dosing, Administration, and Clinical Protocols
Peptide Reconstitution Protocol: Step-by-Step Guide for Prescribers
How to Dose and Titrate Peptide Therapies
When starting peptide therapies, it’s best to begin with a low dose and gradually increase it. For example, with GLP-1 receptor agonists like semaglutide, dosing typically starts at 0.25 mg subcutaneously once a week, increasing every four weeks until reaching a maintenance dose of 2.4 mg weekly. Every dosing decision should be carefully tailored based on a thorough clinical evaluation. As Dr. Kent Bradley emphasizes:
"Work with a clinician who provides a baseline of biomarkers before you introduce peptides. You will need to know where you're starting in order to measure the impact."
Here’s a quick guide to starting doses and key monitoring markers for common peptide classes:
| Peptide Class | Starting Dose | Primary Monitoring Markers |
|---|---|---|
| Semaglutide | 0.25 mg weekly (subcutaneous) | HbA1c, weight, gastrointestinal tolerance |
| Sermorelin | 200–500 mcg nightly | IGF-1, fasting glucose, HbA1c |
| Thymosin Alpha-1 | 1.6 mg twice weekly | CBC with differential, CMP, viral markers |
| TB-500 | 2–5 mg weekly | Clinical markers of tissue repair |
Peptide treatments are seldom intended to be ongoing indefinitely. For instance, growth hormone secretagogues are often cycled, typically for three to six months, followed by a one- to two-month break before reassessment. Dr. Amanda Kahn advises:
"Peptides should be cycled, paused and re-assessed - don't 'set it and let it go.'"
Once dosing is established, proper administration becomes key to ensuring the treatment’s effectiveness.
Administration Methods and Patient Education
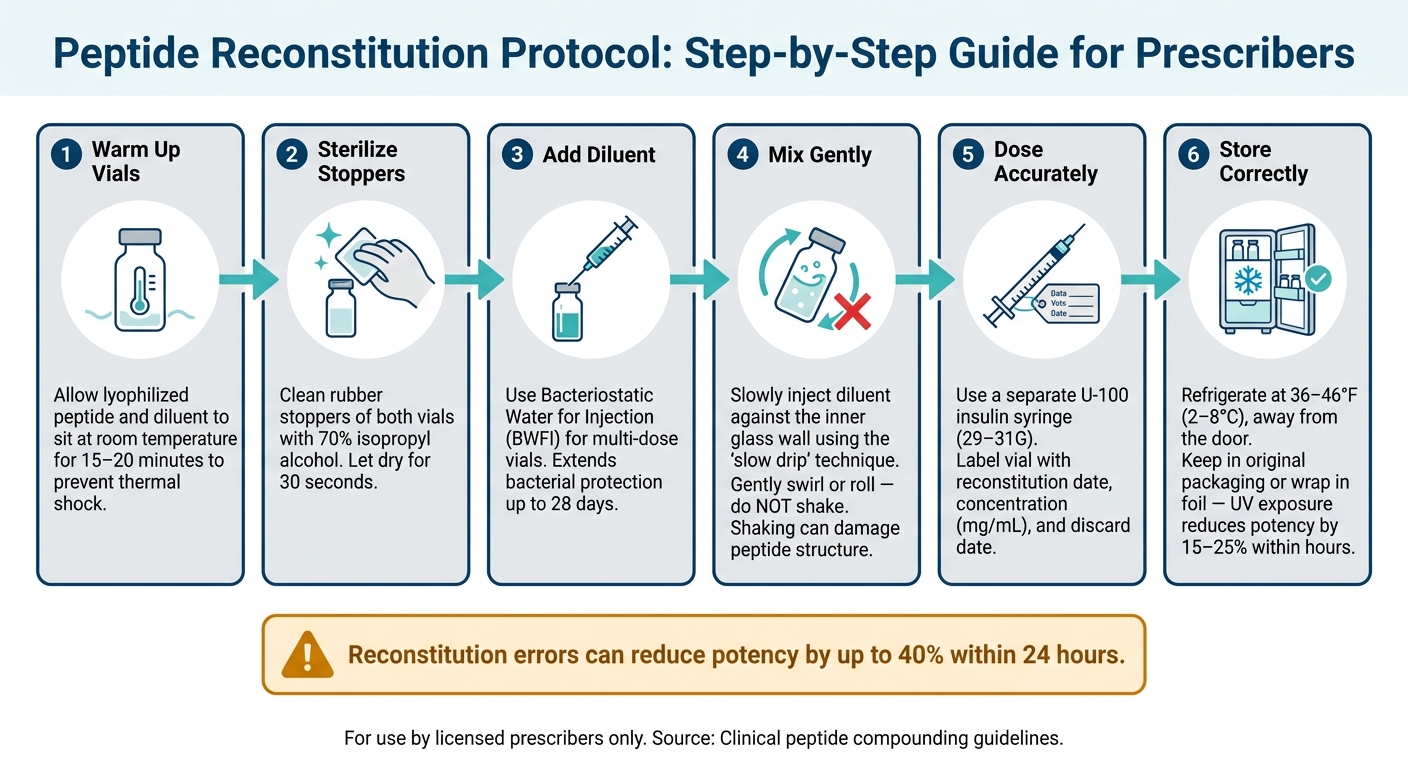
Subcutaneous injection is the most common administration method, but some peptides may be delivered intranasally or orally. For injectable peptides, reconstitution is a critical step, as errors in this process can reduce potency by as much as 40% within 24 hours.
Follow these steps for proper reconstitution:
- Allow both the lyophilized peptide and diluent to sit at room temperature for 15–20 minutes to avoid thermal shock.
- Clean the rubber stoppers of both vials with 70% isopropyl alcohol and let them dry for 30 seconds.
- Use Bacteriostatic Water for Injection (BWFI) as the diluent for multi-dose vials. This extends bacterial protection for up to 28 days.
- Slowly inject the diluent against the inner glass wall using the "slow drip" technique. Gently swirl or roll the vial to mix - avoid shaking, as this can damage the peptide structure.
- Use a separate U-100 insulin syringe (29–31G) for dosing, and label the vial with the reconstitution date, concentration (mg/mL), and discard date.
- Store reconstituted peptides in a refrigerator at 36–46°F (2–8°C), away from the door to prevent temperature fluctuations. Since many peptides are sensitive to light, keep them in their original packaging or wrap them in foil to avoid UV degradation, which can reduce potency by 15–25% within hours.
Counseling patients on injection technique ensures proper preparation and storage, which are essential for maintaining treatment effectiveness.
What to Monitor for Safety and Effectiveness
After establishing proper dosing and administration, monitoring becomes essential to ensure both safety and effectiveness. Each peptide targets specific systems, so monitoring should align with the therapy’s purpose. For growth hormone secretagogues like Sermorelin or Ipamorelin, initial labs should include IGF-1, fasting glucose, and HbA1c. Recheck IGF-1 and fasting glucose after 8–12 weeks, and watch for signs of elevated growth hormone activity, such as edema, joint pain, or carpal tunnel symptoms.
For GLP-1 therapies, monitor HbA1c at six months, and check fasting glucose and weight at every visit. Be aware that nausea affects 20–44% of patients on GLP-1 receptor agonists, with the highest rates seen at a 15 mg dose of tirzepatide. Additionally, gallbladder disease occurs in about 2–3% of patients in clinical trials. Schedule the first follow-up at 4–6 weeks, with lab retesting at 8–12 weeks.
Dr. James Okafor, PharmD, highlights a key concern in peptide therapy:
"The largest safety risk in peptide therapy is provider and product quality - fake or impure compounds from unregulated sources, and prescribers who don't monitor appropriately, cause more harm than the compounds themselves."
For immune peptides like Thymosin Alpha-1, recheck a CBC with differential and a comprehensive metabolic panel (CMP) at 8–12 weeks, while also monitoring infection frequency and inflammatory markers. For tissue repair peptides such as TB-500, clinical outcomes like range of motion, pain levels, and functional scores are the primary focus, though lab tests may be needed depending on the patient’s underlying conditions.
Thorough monitoring is a cornerstone of safe and effective peptide therapy.
sbb-itb-7164bd9
Safety Considerations and Risk Reduction
Common Side Effects and How to Handle Them
Peptide therapy often comes with predictable side effects. For instance, gastrointestinal issues like nausea, vomiting, diarrhea, and constipation are frequently linked to GLP-1 receptor agonists, such as semaglutide and tirzepatide. To ease these symptoms, a slow increase in dosage over several weeks is recommended. Additionally, encouraging patients to eat smaller meals during this period can make a noticeable difference.
Growth hormone secretagogues, including Ipamorelin and MK-677, bring their own set of challenges. Common complaints include water retention, joint discomfort, and mild insulin resistance. These issues are often dose-dependent and may be resolved with a slight reduction in dosage or a brief pause in treatment. It's also worth noting that these peptides can influence T4-to-T3 conversion, which might necessitate adjustments in levothyroxine dosages.
Here’s a quick overview of common side effects and how to manage them:
| Peptide Class | Common Side Effects | Management Strategy |
|---|---|---|
| GLP-1 Agonists | Nausea, vomiting, diarrhea, constipation | Gradual dose titration; smaller meals |
| GH Secretagogues | Edema, joint pain, insulin resistance | Lower dosage; cycling protocols; monitor glucose levels |
| Healing Peptides | Injection site reactions, mild fatigue | Rotate injection sites; watch for infection |
| Melanocortins (PT-141) | Flushing, temporary blood pressure spikes, nausea | Monitor blood pressure; adjust dosing |
Injection-site reactions - like redness, swelling, or irritation - are common across all injectable peptides. These are generally mild and can be minimized by rotating injection sites consistently.
Beyond managing side effects, clinicians must also address the complexities tied to off-label peptide use.
Managing Off-Label Use Responsibly
Off-label peptide use presents unique challenges. Many peptides used in clinical practice are not FDA-approved for their intended applications; instead, they are accessed through compounding pharmacies, which differs from standard off-label prescribing. Informed consent is crucial here. Patients need to understand that these peptides are not FDA-approved, that long-term safety data is limited, and that some level of experimental risk is involved. Importantly, this conversation should be documented in progress notes rather than relying solely on a signed consent form.
Dr. Jossy Onwude, MD, emphasizes this point:
"If the entire process ends at checkout, it is commerce, not care."
Documentation should also justify the medical necessity of the chosen peptide. This includes explaining why it was selected for the patient and why conventional alternatives were insufficient. If an FDA-approved version of the peptide exists, such as Vyleesi for PT-141, it should be the first option. Additionally, clinicians working with athletes must be aware that many peptides, like BPC-157 and GHRPs, are on the WADA Prohibited List, regardless of the intent behind their use.
Ensuring the quality and safety of peptides is another critical aspect of responsible prescribing.
Sourcing Safe, Quality Peptide Products
The effectiveness of peptide therapy hinges on sourcing high-quality products. Approximately 12.5% of peptide providers have been found to use falsified or unverifiable Certificates of Analysis (COA). A legitimate COA should be lot-specific and include third-party testing for potency, purity, sterility, and endotoxins.
Clinicians should source peptides exclusively from 503A or 503B licensed facilities. A 503A pharmacy compounds medications for individual patients based on valid prescriptions and is regulated by state pharmacy boards. In contrast, a 503B outsourcing facility is FDA-registered, adheres to cGMP standards, and can produce larger batches for office use. To verify a facility's legitimacy, clinicians can use the FDA's searchable database and look for PCAB accreditation as an additional quality indicator.
Avoid suppliers offering peptides labeled "not for human use" or "for research purposes only." Dr. Yoon Hang "John" Kim, MD, MPH, warns:
"The legal supply chain for these peptides has been severed at the source. If a licensed 503A pharmacy cannot legally compound them, any clinic obtaining these substances is almost certainly sourcing from research-chemical suppliers."
Using such products deviates from standard care and increases malpractice risks. Regulatory scrutiny is intensifying. As of early 2026, the FDA has reclassified several peptides, including BPC-157, CJC-1295, Ipamorelin, and TB-500, into Category 2 due to safety concerns. Enforcement actions against clinics using research-grade peptides have also increased. Staying updated with the FDA Regulatory Quick Reference and the Bulks List is an essential part of prescribing peptides responsibly.
U.S. Regulatory and Compliance Requirements
How the FDA Regulates Peptide Therapies
Under the Federal Food, Drug, and Cosmetic Act, peptides are categorized as drugs or biologics and fall under the FDA's regulatory umbrella. This means the FDA oversees their manufacturing, labeling, and distribution. However, the FDA does not regulate the practice of medicine, leaving licensed clinicians free to prescribe legal substances based on their professional judgment.
When it comes to compounded peptides, there are two distinct regulatory pathways:
- 503A Pharmacies: These pharmacies compound medications for individual patients based on valid prescriptions. They operate under the supervision of state pharmacy boards.
- 503B Outsourcing Facilities: These are FDA-registered facilities that follow cGMP standards. They can prepare office-use batches without requiring patient-specific prescriptions.
For a substance to be used in compounding, it must meet one of the following criteria: have a USP/NF monograph, be an ingredient in an FDA-approved drug, or appear on the FDA's official Bulks Lists.
In September 2023, the FDA introduced stricter regulations by reclassifying 19 peptides - such as BPC-157, TB-500, CJC-1295, and Ipamorelin - to Category 2 due to safety concerns, effectively barring their routine compounding. The FDA is currently reviewing 14 of these peptides for potential reclassification to Category 1, with an advisory committee meeting scheduled for July 23–24, 2026. Clinicians should keep an eye on the Federal Register for updates.
Recent enforcement actions highlight the changing regulatory environment. For example, in March 2026, the FDA issued warning letters to telehealth companies for unlawfully marketing compounded GLP-1 drugs. Similarly, in January 2026, an operator from Paradigm Peptides pled guilty to shipping unapproved peptide products, including BPC-157 and TB-500.
"The RUO label does not protect against regulatory enforcement, and the absence of enforcement yesterday is no guarantee of tolerance tomorrow." - Abha Kundi, Counsel, ArentFox Schiff
These developments highlight the importance of thorough legal documentation and adherence to regulations.
Legal and Documentation Obligations for Prescribers
Beyond regulatory compliance, clinicians must meet stringent legal documentation standards. This involves maintaining detailed records for every peptide prescription, which must stem from a valid physician-patient relationship. Even virtual consultations must include a genuine clinical encounter. The medical record should clearly justify why FDA-approved treatments were not suitable for the patient.
Informed consent is more than just a signed form. Clinicians should document detailed conversations where patients acknowledge the compounded nature of the peptide, understand the lack of FDA approval, are aware of experimental risks, and are informed of alternative treatments. As Nick Locascio of Conviction Labs puts it:
"If your notes look identical for every BPC-157 prescription, you're doing it wrong."
Additionally, prescribers should confirm in writing that their malpractice insurance covers compounded or unapproved substances. State-specific rules may also apply, with some states (e.g., California) imposing stricter requirements than federal standards.
The table below outlines key documentation elements every prescriber should maintain:
| Documentation Element | What It Must Include |
|---|---|
| Medical Necessity | Explanation of why FDA-approved treatments are unsuitable for the patient |
| Informed Consent | Disclosure of compounded status, lack of FDA approval, risks, and alternatives |
| Baseline Labs | Relevant tests (e.g., IGF-1 for growth hormone peptides, HbA1c for diabetes-related peptides, CBC for immune-related peptides) |
| Pharmacy COA | Batch-specific Certificate of Analysis verifying potency, purity, and sterility |
| Follow-up Notes | Justification for continuing, adjusting, or discontinuing therapy |
Maintaining these records not only ensures compliance but also integrates seamlessly into established treatment protocols.
Clinical Tools That Support Practice Integration
Compliance doesn't have to slow down your workflow. Leveraging structured EMR templates can help ensure all necessary documentation - such as medical necessity, contraindication screenings, and informed consent - is captured during patient visits. Tools like reconstitution calculators and unit conversion aids can also reduce dosing errors and streamline the process.
Platforms like PeptidePrescriber offer free clinical tools to simplify the integration of peptide therapies into your practice. Their resources include a reconstitution calculator, a dosing protocol library, an injection site guide, and unit conversion tools. For teams, their Starter Pack provides editable consent templates and a regulatory quick reference to standardize workflows.
For pharmacy verification, the FDA's searchable 503B facility database is a valuable tool. Pharmacies with PCAB or ACHC accreditation often adhere to higher quality standards. Combining these tools with consistent documentation practices will help build a compliant and defensible approach to peptide therapy.
Conclusion: Building a Sound Peptide Therapy Practice
Establishing a successful peptide therapy practice requires a strong grasp of clinical protocols, safety measures, and the ever-changing regulatory environment. With the peptide therapeutics market growing rapidly, licensed prescribers face both exciting opportunities and significant responsibilities.
The cornerstones of a reliable practice are evidence-based knowledge, safe sourcing, and thorough documentation. Use an evidence-grading framework to separate well-researched peptides from experimental ones. Always source peptides from licensed 503A or 503B pharmacies and request a batch-specific Certificate of Analysis for every order. Comprehensive documentation - including medical necessity, informed consent, baseline labs, and follow-up notes - is essential to safeguard your patients and your license. These practices, combined with precise dosing and close monitoring, ensure safe and effective treatment.
The regulatory environment is also evolving quickly. For example, on April 15, 2026, the FDA removed BPC-157, TB-500, and KPV from the Category 2 restricted list. However, these peptides are still subject to the PCAC advisory meeting scheduled for July 23–24, 2026. Staying informed through Federal Register updates is no longer optional - it’s a critical part of clinical practice.
"Regulatory actions, not political commentary, directly impact clinical practice." - LumaLex Law
To streamline your peptide program, practical tools can make a big difference. PeptidePrescriber offers free resources like a reconstitution calculator, dosing protocol library, injection site guide, and an AI-powered research assistant tailored for licensed prescribers. Their Starter Pack includes editable consent templates and a regulatory quick reference guide, helping you standardize your workflow from the start. All protocols are sourced from PubMed and updated monthly.
"Peptide prescribing clarity - without the sales pitch." - PeptidePrescriber
FAQs
What baseline labs should I order before starting peptide therapy?
Baseline labs are essential for ensuring safety, confirming a patient’s suitability, and monitoring their progress. A typical panel includes a Comprehensive Metabolic Panel (CMP), Complete Blood Count (CBC), a lipid panel, and important markers like fasting glucose, insulin, and HbA1c. It’s also a good idea to include a thyroid panel (covering TSH, free T3, and T4). For certain peptides, you may need tests like IGF-1 or lipase/amylase. Reviewing the individual’s medical history can help determine if additional tests, such as hormone panels, might be necessary.
How do I choose between a 503A pharmacy and a 503B outsourcing facility?
Choosing between a 503A pharmacy and a 503B outsourcing facility comes down to your specific medical requirements.
A 503A pharmacy is ideal for creating custom medications tailored to individual patients. They prepare these formulations based on valid prescriptions and operate under state regulations.
On the other hand, a 503B outsourcing facility is the better choice when you need a stock of medications for in-office use. These facilities are registered with the FDA, adhere to rigorous cGMP standards, and are subject to regular federal inspections.
What documentation protects me most when prescribing compounded peptides?
To safeguard yourself legally, make sure to establish a proper physician-patient relationship and keep thorough, personalized records. Clearly note the clinical reasoning and medical need for choosing a compounded product over a commercially available option. Your documentation should include informed consent, the patient’s medical history, and specific reasons why conventional treatments were not appropriate. Additionally, ensure that all compounded medications come from state-licensed 503A pharmacies or FDA-registered 503B outsourcing facilities.