Navigating compounded peptide regulations in 2026 has become more stringent due to recent FDA updates. Here's what you need to know:
- Clinical Need Standard: Compounding is only allowed when FDA-approved drugs are unsuitable for specific patients, with documented clinical justification required.
- 503A vs. 503B Rules: Pharmacies under 503A need patient-specific prescriptions, while 503B facilities can produce office stock but face stricter manufacturing and reporting requirements.
- Regulatory Changes: On April 22, 2026, the FDA removed 12 peptides, including BPC-157 and TB-500, from the "Do Not Compound" list. However, these peptides are not yet fully approved for compounding and await further review in July 2026.
- GLP-1 Peptides Restrictions: Semaglutide and others are now off the shortage list, restricting large-scale compounding unless a documented clinical difference exists.
- Compliance Risks: Using research-grade peptides or marketing compounded drugs as equivalents to FDA-approved products can lead to legal consequences.
- Best Practices: Verify API sources, document clinical necessity, and stay updated on regulatory shifts by monitoring FDA announcements and the Bulk Drug Substances lists.
Understanding and adhering to these rules is critical to avoid penalties and ensure patient safety.
11 Peptides Just Got Greenlit by the FDA (Here's What Changed)
sbb-itb-7164bd9
Key FDA Guidelines for Compounded Peptides
503A vs. 503B Compounding: FDA Compliance Guide 2026
Understanding FDA compliance starts with two critical sections of the Federal Food, Drug, and Cosmetic Act: 503A and 503B. These sections outline distinct pathways for compounding, each with unique rules, oversight, and limitations. Whether you're a prescriber or pharmacist, knowing which pathway applies to your practice is essential for staying within legal boundaries.
Sections 503A and 503B: What Prescribers Need to Know
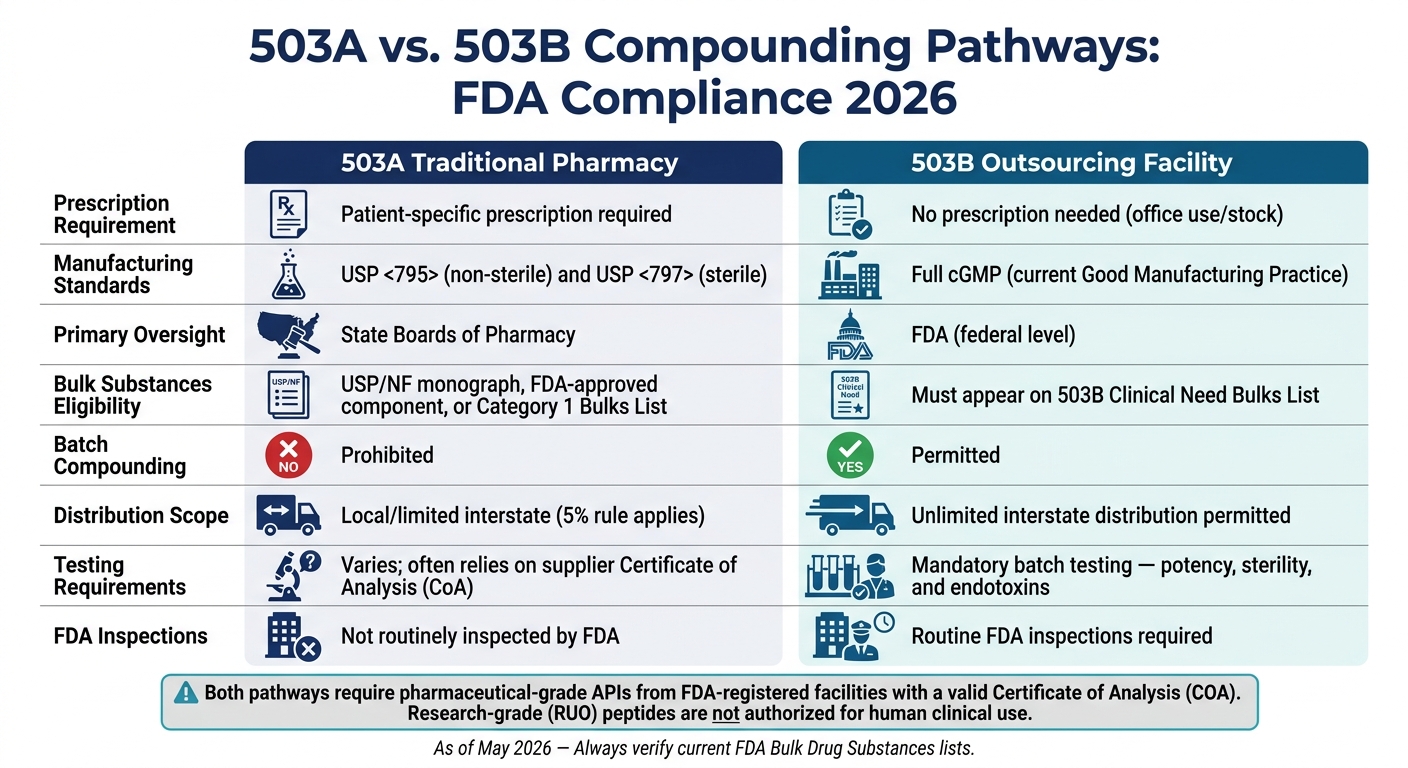
Section 503A governs traditional pharmacies and physician offices. Under this framework, each compound must be prepared for a specific patient with a valid prescription. While these pharmacies are exempt from FDA current Good Manufacturing Practice (cGMP) requirements, they must adhere to USP <795> (non-sterile compounding) and USP <797> (sterile compounding) standards. Oversight primarily falls to state boards of pharmacy, not the FDA.
Section 503B, on the other hand, applies to FDA-registered outsourcing facilities. These facilities can produce larger batches without requiring patient-specific prescriptions, often referred to as "office stock." However, this flexibility comes with stricter requirements, including full cGMP compliance, routine FDA inspections, and mandatory reporting of adverse events.
| Feature | 503A (Traditional Pharmacy) | 503B (Outsourcing Facility) |
|---|---|---|
| Prescription Requirement | Patient-specific prescription required | No prescription needed (office use) |
| Manufacturing Standards | USP <795> and <797> | cGMP |
| Primary Oversight | State Boards of Pharmacy | FDA (federal) |
| Bulk Substances | USP/NF monograph, approved drug component, or 503A Bulks List | Must appear on 503B Clinical Need Bulks List |
| Batch Compounding | Prohibited | Permitted |
As the Peptide Association has emphasized:
"Prescribing substances that cannot be lawfully compounded under either 503A or 503B frameworks is a different matter entirely [than off-label prescribing]."
Next, let’s examine how upcoming classification updates will influence compounding practices.
2026 Updates to Peptide Classification
One of the major regulatory shifts in 2026 occurred on April 22, 2026, when the FDA removed 12 peptides from Category 2 of the interim 503A Bulks List. These peptides include: BPC-157, TB-500, KPV, MOTs-C, Semax, Epitalon, Melanotan II, Emideltide (DSIP), Cathelicidin LL-37, Dihexa Acetate, GHK-Cu (injectable), and PEG-MGF.
This removal is notable but doesn't mean these peptides are automatically cleared for compounding. While the explicit prohibition has been lifted, these substances must be formally added to Category 1 of the 503A Bulks List before they can be compounded legally. The Pharmacy Compounding Advisory Committee (PCAC) is set to meet on July 23–24, 2026, to evaluate seven of these peptides: BPC-157, KPV, TB-500, MOTs-C, DSIP, Semax, and Epitalon.
For GLP-1 peptides, the situation is more restrictive. As of April 30, 2026, the FDA proposed removing semaglutide, tirzepatide, and liraglutide from the 503B Bulks List, citing resolved drug shortages. This effectively ends large-scale compounding of these peptides.
Core Legal Tests for Compliance
To comply with FDA guidelines, compounded peptides under both 503A and 503B must meet three key legal tests:
- Bulk Substance Criteria: The active ingredient must either have a USP/NF monograph, be an FDA-approved component, or appear on the applicable Bulks List (Category 1 for 503A or the Clinical Need list for 503B).
- Clinical Necessity: Compounding is allowed only when an FDA-approved drug is unsuitable for a specific patient. This must be documented at the individual level.
- No Duplication of Approved Drugs: A compounded peptide cannot replicate an FDA-approved drug unless a prescriber documents a substantial difference for the patient, such as removing an allergen or creating a dosage form not commercially available. This rule halted large-scale compounding of semaglutide after the drug shortage ended.
One universal requirement is the use of pharmaceutical-grade active pharmaceutical ingredients (APIs). Every API must come from an FDA-registered facility with a valid Certificate of Analysis (COA). Research-grade peptides, regardless of their claimed purity, are not authorized for clinical use in humans.
Compliance Workflows for Healthcare Professionals
Creating effective compliance workflows means finding the right balance between meeting strict regulatory standards and ensuring efficient patient care.
Patient-Specific Requirements Under 503A
When working under 503A guidelines, every prescription must be tied to a specific, identified patient - no pre-made batches sitting on shelves. Before submitting a 503A prescription, verify that the pharmacy holds a valid state license in both its home state and the state where your patient resides. Additionally, confirm that the active ingredient is listed on the Category 1 Bulks List or is part of an FDA-approved drug.
If the prescription involves a compounded version of an approved drug, there must be a documented clinical rationale, such as an allergy or the need for a dosage form that isn’t commercially available. As HolistiCare emphasizes:
"Patient preference or cost are NOT acceptable rationales under current FDA interpretation. The clinical necessity must be documented."
503B Outsourcing Facility Standards
For peptides or other compounds intended for office use - where prescriptions aren’t tied to specific patients - you’re operating under 503B rules. This is only permissible if the facility is registered with the FDA as an outsourcing facility and the substance is on the 503B Bulks List. Before ordering, confirm the facility’s FDA registration and check its inspection history in the FDA database. Facilities with unresolved FDA observations could pose compliance risks.
Also, ensure the peptide you’re ordering is eligible for compounding. Substances on the Category 2 restricted list are off-limits. Additionally, 503B facilities cannot produce compounds that are “essentially a copy” of commercially available drugs. For instance, once the FDA resolves a drug shortage, mass compounding of that drug becomes illegal. This occurred with semaglutide and tirzepatide, leaving compounders without legal grounds to continue production.
Incorporating these checks into your daily workflows can help ensure alignment with FDA regulations.
Aligning Clinical Practice with FDA Standards
To maintain compliance, your daily routines should reflect regulatory requirements. This includes verifying sourcing, documenting clinical necessity, and staying updated on changes to the Bulks List.
When sourcing, always request a Certificate of Analysis (COA) that confirms potency, purity, sterility, and endotoxin levels. A missing COA is a red flag. Ensure that the active pharmaceutical ingredient (API) is pharmaceutical-grade and comes from an FDA-registered facility. Avoid APIs labeled "Research Use Only" (RUO). As Abha Kundi, Counsel and Longevity & Healthspan Industry Group Co-Leader, explains:
"The RUO label is not a protective regulatory force field, and the absence of enforcement yesterday is no guarantee of tolerance tomorrow."
Every patient chart should clearly document the clinical rationale for compounding, the patient’s specific needs, and the necessity of the compounded formulation. It’s also vital to monitor the Federal Register regularly since peptide classifications can shift without much notice. For example, the upcoming PCAC meeting on July 23–24, 2026, could result in changes to the status of compounds like BPC-157, KPV, and TB-500. Reviewing your formulary after such regulatory events helps prevent compliance gaps.
Common Regulatory Risks and How to Avoid Them
When it comes to compliance with compounded peptides, even well-meaning prescribers can find themselves in trouble. The risks aren’t always obvious, and many issues arise not from bad intentions but from misunderstandings about what’s actually allowed. Let’s dive into the common pitfalls and how to steer clear of them.
Gray-Market Sourcing and Noncompliant Ingredients
One major trap is sourcing peptides from suppliers who label their products as "Research Use Only" (RUO) to dodge legal scrutiny. The FDA doesn’t buy this excuse. For example, in March 2026, the agency issued Warning Letter Ref. 721806 to Bernard Gramlich of Gram Peptides. His company sold Retatrutide and Tirzepatide with RUO labels, while openly marketing them for appetite suppression and weight management. The RUO label offered no protection.
Gray-market sourcing can lead to serious consequences, including hefty fines and even guilty pleas. Worse, malpractice insurance often excludes claims tied to unapproved or noncompliant drugs.
"If a product is labeled 'not for human use,' administering it to a human patient is an indefensible practice. No disclaimer on a supplier's website transfers liability away from the treating physician." - Yoon Hang "John" Kim, MD, MPH
The solution? Stick to FDA-registered suppliers. Use the FDA’s searchable database to verify pharmacy registration and inspection history before making any purchases. Always ensure you’re ordering pharmaceutical-grade active pharmaceutical ingredients (API) from an FDA-registered facility. Staying vigilant about sourcing will help you avoid unnecessary risks.
Copy-Product Compounding Restrictions
Compounding a drug that’s essentially a copy of a commercially available medication is prohibited under both 503A and 503B regulations - unless the drug is on the FDA’s shortage list or there’s a documented clinical reason the patient can’t use the commercial version. Ignoring this rule can lead to immediate legal trouble.
For instance, when the FDA declared the tirzepatide shortage resolved in late 2024, compounders who continued producing tirzepatide copies became legally exposed. By March 2026, the FDA issued 30 warning letters to telehealth companies marketing compounded GLP-1 products, claiming they were equivalent to FDA-approved drugs like Ozempic and Mounjaro.
Here’s how to avoid this risk:
- Avoid marketing compounded drugs as equivalents to FDA-approved products.
- Regularly review your marketing materials to ensure they don’t imply "sameness" to brand-name drugs.
- Document the clinical rationale for every patient receiving a compounded version of a drug with a commercial counterpart.
Staying proactive with these steps can help protect your practice against regulatory scrutiny.
Keeping Up with FDA Rulemaking and Shortage Updates
The regulatory landscape for peptides is constantly shifting, which makes staying informed a key part of compliance. For example, in April 2026, the FDA removed 12 peptide substances, including BPC-157, TB-500, and Semax, from the Category 2 "Do Not Compound" list. However, this doesn’t mean they’re fully approved for compounding. These peptides remain in limbo until the FDA explicitly grants enforcement discretion, which could take months or even years. The PCAC meeting scheduled for July 23–24, 2026, may provide further clarity.
Here’s a snapshot of the current status of some high-profile peptides as of May 2026:
| Peptide | Current Status | Compounding Permitted? |
|---|---|---|
| BPC-157, TB-500 | Removed from Category 2 | Not yet; pending PCAC review (July 2026) |
| Semaglutide | Commercially available, off shortage | Generally prohibited |
| Tirzepatide | Commercially available, off shortage | Generally prohibited |
| GHK-Cu (Injectable) | Removed from Category 2 | Pending PCAC consultation (Feb 2027) |
| Research-grade peptides | Uncategorized / RUO | Illegal for human use |
To avoid compliance gaps, schedule quarterly formulary reviews. Regularly check the FDA Federal Register and the 503A/503B Bulk Drug Substances lists. Don’t wait for updates to reach you - what was allowed last quarter might not be allowed today.
"The real question... is whether the FDA will extend enforcement discretion to these substances, allowing them to be compounded under the interim policy while the formal rulemaking process plays out." - Guilherme Ferrari Faviero, Senior Associate, Frier Levitt
Incorporating this habit into your practice calendar can help you stay ahead of regulatory changes and avoid enforcement actions that could impact your patients or your license.
Tools and Resources for Compliant Peptide Compounding
Ensuring compliance in peptide compounding isn't just about understanding the regulations - it’s about having the proper tools and resources to implement them effectively. Fortunately, there are several resources available to help streamline this process.
Clinical Tools That Support Compliance
PeptidePrescriber offers a variety of free and premium tools designed to make compliance easier for prescribers. For example:
- The Reconstitution Calculator helps eliminate dosing errors by accurately converting syringe units, which improves patient safety.
- evidence-based dosing protocols provide well-documented clinical guidelines for prescribing peptides.
- The AI-powered research assistant allows prescribers to quickly search peptide monographs, saving time compared to sifting through scattered research.
For those new to peptide prescribing, the Prescriber Starter Pack is especially helpful. It includes editable consent templates, a regulatory quick reference guide, and an implementation checklist - all designed to help build a compliance-ready workflow from the start. A 2026 study on insulin safety protocols found that standardized tools like these significantly improved healthcare professionals’ proficiency, increasing it from 32% to 70%.
"Quality assurance in peptide therapy is not an administrative burden. It is a core clinical responsibility." - Peptide Association
Another valuable resource is the Peptide Science Institute (PSI). As of May 2026, PSI monitors the regulatory status of 147 peptide compounds, including PCAC review schedules and Category 1/2 classifications. When sourcing peptides, the FDA's searchable database of registered 503B outsourcing facilities is an essential tool. It allows you to verify a facility’s registration and inspection history, ensuring your sources meet compliance standards.
For a better understanding of operational differences, the comparison between 503A and 503B facilities below is a useful guide.
503A vs. 503B: Side-by-Side Comparison
| Feature | 503A (Traditional Pharmacy) | 503B (Outsourcing Facility) |
|---|---|---|
| Distribution Scope | Local/limited interstate (5% rule applies) | Unlimited interstate distribution permitted |
| Testing Requirements | Varies; often relies on supplier CoA | Mandatory batch testing - potency, sterility, and endotoxins |
If you’re sourcing from a 503B facility, you benefit from greater distribution flexibility and access to larger batches. However, these facilities must adhere to cGMP standards. For 503A pharmacies, peptides must be on the Category 1 Bulks List and tied to a patient-specific prescription.
With this framework in mind, it’s critical to stay informed on the current regulatory status of individual peptides.
Peptide Status and Compounding Pathways
Understanding the regulatory status of peptides is crucial for staying compliant with FDA guidelines. The table below outlines the compounding status of several peptides as of May 2026:
| Peptide | Current Regulatory Status | Compounding Pathway |
|---|---|---|
| Sermorelin | Category 1 | Compoundable via 503A with prescription |
| NAD+ | Category 1 | Compoundable via 503A with prescription |
| PT-141 | FDA-Approved (Vyleesi) | Compoundable for off-label use |
| BPC-157 | Removed from Category 2 (April 2026) | Not yet compoundable; awaiting PCAC review July 2026 |
| Semaglutide | FDA-Approved; shortage resolved | Restricted; requires documented clinical difference |
| CJC-1295 | PCAC voted against (late 2024) | Not compoundable |
| AOD-9604 | PCAC voted against (December 2024) | Not compoundable |
"Removal from Category 2 is not the same as authorization to compound - the FDA must add [the peptide] to the 503A bulks list through formal rulemaking... before licensed compounding pharmacies can legally produce it." - PeptideClarity Regulatory Tracker
This table serves as a starting point, but it’s essential to regularly cross-check it with the FDA's Bulk Drug Substances lists and updates in the Federal Register to ensure compliance.
Conclusion: Building a Compliant Peptide Therapy Practice
Navigating the regulations for compounded peptides in 2026 is no easy task. The upcoming PCAC meeting on July 23–24, 2026, will play a critical role in determining the future of seven peptides, including BPC-157 and TB-500. As Scott Brunner, CEO of the Alliance for Pharmacy Compounding, aptly stated:
"Even if FDA acted tomorrow, pharmacies would still have to turn away those prescriptions because they couldn't acquire the compliant API to prepare the drugs."
This highlights the operational hurdles that pharmacies face today. Maintaining compliance requires pharmacies to stay vigilant - ensuring API sources are verified, prescriptions are tied to specific patients, and peptide categories are checked before prescribing. Sourcing pharmaceutical-grade API from FDA-registered facilities and adhering to 503A requirements remain essential.
The FDA's enforcement actions add further pressure. In the 12 months ending March 2026, the agency issued over 80 Warning Letters to telehealth companies, with 30 of those issued in a single month. This demonstrates the FDA’s focus on addressing marketing violations and gray-market sourcing. As Charles D. Snow and Karla L. Palmer observed on the FDA Law Blog:
"The window for unregulated gray-market peptides may be closing, but the window for regulated compounded peptides is not yet fully open."
FAQs
What documentation proves “clinical need” for a compounded peptide?
To demonstrate "clinical need" for a compounded peptide, providers are required to document the following:
- Individualized medical necessity: Clearly outline why the specific patient requires the compounded peptide.
- Limitations of commercial alternatives: Explain why available commercial options are either inadequate or contraindicated for the patient.
- Informed consent and monitoring plans: Provide evidence that the patient was informed about the treatment and that appropriate monitoring measures are in place.
This documentation ensures adherence to FDA guidelines while focusing on the patient's unique medical requirements.
How do I decide whether 503A or 503B applies to my peptide order?
To figure out whether 503A or 503B applies, start by identifying the purpose and source of the peptide. If it’s prepared specifically for an individual patient and comes from a licensed pharmacy, it falls under 503A. On the other hand, if it’s produced in bulk by an FDA-registered outsourcing facility, it’s classified under 503B.
It’s also important to check the peptide’s regulatory status. Look into whether it’s included on the FDA’s bulks list or falls under restricted categories. This step ensures everything aligns with the appropriate compliance rules.
If a peptide is removed from the 'Do Not Compound' list, is it legal to compound?
When a peptide is removed from the 'Do Not Compound' list, it doesn't mean it's automatically allowed for compounding. Its status remains unclear until the FDA officially reclassifies it as suitable for compounding. This process involves further review and potential approval. Always check the latest FDA guidelines to ensure you're operating within the rules.