
Peptide therapies are reshaping clinical care in 2026, with advancements across weight management, regenerative medicine, neurocognition, aesthetics, and immunomodulation. Here’s a quick overview:
- Weight Loss Breakthroughs: Retatrutide achieved up to 30% weight loss in trials, rivaling bariatric surgery. CagriSema and high-dose oral semaglutide also showed promising results.
- Regenerative Medicine: BPC-157 and TB-500 show potential for tissue repair but lack large-scale human trials. Safety concerns persist due to unregulated markets.
- Neurocognition: Semax, Selank, and Cerebrolysin are gaining attention for cognitive and mood support, with new dosing strategies like intranasal delivery.
- Aesthetics: Oral peptides like BCP improve skin hydration and wrinkle reduction, outperforming topical options. GHK-Cu and Argireline offer targeted benefits.
- Immunomodulation: Oral peptides like Icotrokinra for psoriasis and PEPITEM for arthritis are emerging as alternatives to biologics.
Regulatory Updates: The FDA is tightening rules on compounded peptides, with key reviews scheduled for later in 2026. Clinicians must adapt to these changes and prioritize sourcing from verified pharmacies.
Stay informed and use evidence-based protocols to integrate peptides safely into practice.
Journal Club #3: Peptide Safety & Efficacy in Sports Medicine (2026 Update)
sbb-itb-7164bd9
GLP-1 and Related Metabolic Peptides: Updates on Weight and Cardiometabolic Care
2026 Weight Loss Peptides Compared: Mechanism, Efficacy & Clinical Use
The years 2025–2026 have brought groundbreaking developments in the GLP-1 space, with new therapies achieving weight loss results once thought possible only through bariatric surgery. At the same time, regulatory changes are reshaping how these medications are prescribed and utilized.
2025–2026 Research Highlights
Retatrutide, Eli Lilly's triple agonist, has delivered unprecedented outcomes in the TRIUMPH-1 Phase 3 trial. Among 2,339 adults with obesity and no diabetes, participants on the 12 mg dose achieved an average weight loss of 28.3% (~70 lbs) over 80 weeks. In an extension study, those with a BMI ≥35 saw their average weight loss climb to 30.3% (85.0 lbs) at 104 weeks, with 65.3% achieving a BMI under 30 by week 80.
"It was impressive to see that every dose of retatrutide resulted in clinically meaningful weight reduction for nearly all participants, and people with severe obesity on the highest dose lost on average 30% of their body weight over two years." - Ania Jastreboff, M.D., Ph.D., Yale School of Medicine
The REDEFINE 1 trial (June 2025) confirmed that CagriSema - a combination of cagrilintide and semaglutide - produced 20.4% weight loss at 68 weeks compared to 3.0% for placebo in a study of 3,417 adults without diabetes. Meanwhile, high-dose oral semaglutide (25 mg) achieved 17% average weight loss in the OASIS 4 trial. A sub-analysis presented at the European Congress on Obesity (May 2026) highlighted even greater success for early responders (≥10% weight loss by week 16), who reached 21.6% by week 64.
A 2026 systematic review emphasized the quality of weight loss achieved with GLP-1 receptor agonists, showing a 17% reduction in fat mass and visceral adipose tissue within the first three months, while lean mass loss remained minimal at about 2%. The BELIEVE Phase 2 trial added to this by combining bimagrumab (an ActRII inhibitor) with semaglutide. Among 507 adults with obesity, the combination led to a 17.8 kg weight loss at 48 weeks, compared to 14.2 kg with semaglutide alone. Notably, 92.2% of the weight loss came from fat mass, preserving muscle.
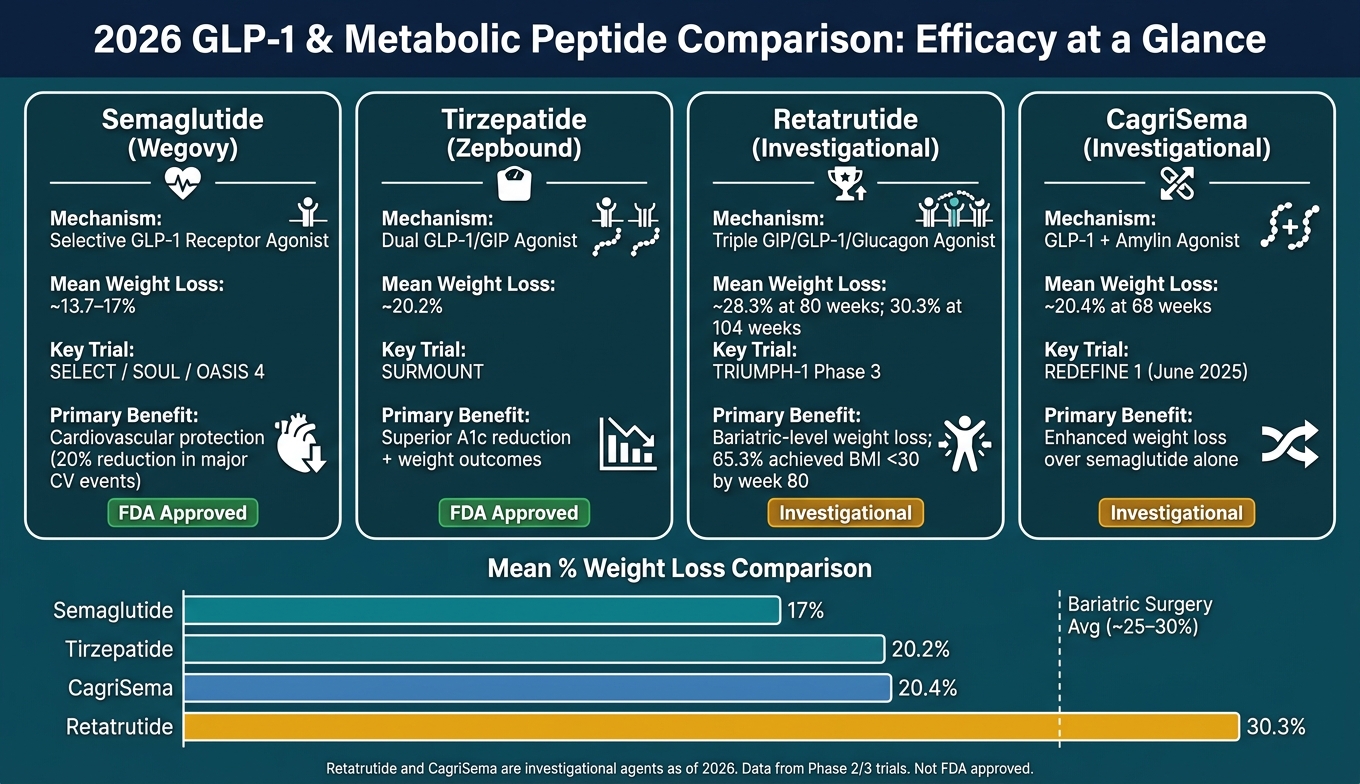
Here’s how the leading agents stack up:
| Agent | Mechanism | Mean Weight Loss | Primary Benefit |
|---|---|---|---|
| Semaglutide (Wegovy) | Selective GLP-1 RA | ~13.7–17% | Cardiovascular protection (SELECT, SOUL) |
| Tirzepatide (Zepbound) | Dual GLP-1/GIP Agonist | ~20.2% | Superior A1c and weight outcomes |
| Retatrutide (Investigational) | Triple GIP/GLP-1/Glucagon | ~28.3% | Bariatric-level weight loss |
| CagriSema (Investigational) | GLP-1 + Amylin Agonist | ~20.4% | Enhanced weight loss over semaglutide alone |
These findings are shaping new safety protocols and regulatory standards.
Safety and Regulatory Updates
Two major regulatory updates in 2026 are worth noting for U.S. clinicians. First, in January 2026, the FDA removed the suicidal ideation and behavior warnings from the labels of Saxenda, Wegovy, and Zepbound, following a meta-analysis of 91 trials involving 107,910 patients that showed no increased risk. Second, as of May 1, 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list, effectively ending large-scale compounding of these medications. Clinicians who rely on compounded formulations will need to adjust their prescribing practices.
In the UK, the MHRA updated product labels in January 2026 to include warnings about rare but severe cases of necrotizing pancreatitis, with 1,296 reported incidents between 2007 and 2025, including 19 fatalities. If pancreatitis is suspected, therapy should be discontinued immediately and not restarted after confirmation. Additionally, the American Society of Anesthesiologists (ASA) continues to advise pausing weekly GLP-1 injectables for 7 days before elective procedures to reduce aspiration risk.
One notable approval this year: the FDA greenlit Foundayo (orforglipron) in April 2026. This is the first non-peptide oral GLP-1 receptor agonist that doesn’t require fasting for administration, and it was approved just 50 days after its filing.
Clinical Application and Protocol Integration
These findings and regulatory updates highlight the need for tailored clinical protocols. Tirzepatide is ideal for patients needing maximum weight loss and glycemic control, while semaglutide remains the go-to for those with established cardiovascular disease, thanks to its proven ability to reduce major cardiovascular events (20% reduction in SELECT, 14% in SOUL).
"Tirzepatide should be prioritized for patients requiring maximal weight and glycemic improvements, whereas semaglutide is currently optimal for those requiring proven cardiovascular event reduction." - Maan H. Harbi, Umm Al-Qura University
For patients at risk of muscle loss, combining GLP-1 therapy with resistance training and high-protein diets is essential. Clinicians using next-generation agents like retatrutide should monitor for temporary ALT elevations during dose titration, which typically resolve by week 24 and are linked to hepatic triglyceride mobilization. Patients with Type 2 diabetes and pre-existing retinopathy should undergo a baseline eye exam before starting therapy, as rapid HbA1c reductions may worsen the condition. These considerations are vital as peptide-based treatments continue to refine the landscape of weight and cardiometabolic care.
Regenerative and Musculoskeletal Peptides: Orthopedics and Sports Medicine Applications
Regenerative peptides are gaining attention in orthopedics and sports medicine, offering new insights into optimizing tissue repair strategies for clinical use.
Emerging Evidence in Tissue Repair
In 2026, researchers uncovered how BPC-157 works: its proline residue at position 3 interacts with FBXO22, stabilizing BACH1 and boosting proangiogenic factors like PDGFB, EGFR, FGF2, and FGFR1. This mechanism supports vascular regeneration in poorly vascularized tissues, such as tendons. A review in JAAOS Global Research & Reviews that same year explored how BPC-157 and TB-500 influence signaling pathways like PI3K/Akt, mTOR, TGF-β, and AMPK, highlighting their potential in musculoskeletal healing.
Animal studies back these findings. In rodent models of muscle contusion, BPC-157 increased microvascular density from 1.7 ± 0.4 to 6.2 ± 3.2 vessels. A small study involving 12 patients found that intra-articular BPC-157 injections relieved chronic knee pain for over six months in 91.6% of participants. While promising, the evidence is still limited - no large-scale randomized controlled trials have been conducted in orthopedic patients as of May 2026.
"The preclinical evidence is compelling... But the clinical evidence gap is significant: no human trials, no FDA approval, and an unregulated market growing far ahead of the science." - Jeremy Burnham, MD, Orthopedic Surgeon
BPC-157 and TB-500 play complementary roles. BPC-157, derived from gastric juice, focuses on angiogenesis and collagen organization via growth factor modulation. Meanwhile, TB-500, a synthetic fragment of Thymosin Beta-4, supports anti-inflammatory pathways and cell migration. Together, these peptides offer intriguing possibilities for tissue repair.
Safety and Doping Considerations
The regulatory landscape for these peptides remains murky. In April 2026, both BPC-157 and TB-500 were removed from the FDA's Category 2 restricted list after withdrawn nominations. However, they are still classified as unapproved drugs, with formal PCAC review set for July 23, 2026, and FDA rulemaking expected in late 2026 or early 2027.
For athletes, things get even trickier. These peptides are prohibited under the WADA Prohibited List, regardless of their FDA status. Clinicians treating competitive athletes must confirm compliance with WADA rules.
The gray market poses additional risks. Analyses of unregulated peptide products have revealed purity levels ranging from 5% to 75%, with some containing harmful contaminants like arsenic and lead. In one case, the DOJ seized $1.79 million worth of unapproved peptides. There’s also a theoretical concern that BPC-157’s pro-angiogenic properties could accelerate undiagnosed malignancies, though this has not been observed in human trials.
"The commercial market for compounded peptides now outpaces supporting clinical evidence. Patients are injecting substances that have never been adequately tested in humans." - Rita Jew, PharmD, MBA, BCPPS, President of ISMP
Given these concerns, clinicians must exercise caution and follow strict protocols when considering these peptides for treatment.
Practical Integration into Treatment Protocols
Before introducing peptides, ensure patients have an accurate diagnosis, follow structured rehabilitation with progressive loading, prioritize sleep, and maintain adequate protein intake (1.6–2.2 g/kg of body weight daily).
"BPC-157 appears to promote healing even in situations where recovery was impaired, such as tissues affected by corticosteroid use or areas with very poor blood supply." - Dr. Christopher S. Raffo, Orthopedic Surgeon
If peptides are used, source them from licensed 503A or 503B pharmacies with valid Certificates of Analysis. Preclinical studies have used daily subcutaneous doses ranging from 10 ng/kg to 10 µg/kg, with some rodent studies in 2026 testing 5–40 µg/kg daily over seven days. Human dosing remains uncertain, but a 2025 pilot study on healthy volunteers reported no adverse effects on heart, kidney, or liver function after intravenous infusions of up to 20 mg of BPC-157. These experimental doses should be approached cautiously and always as an adjunct to physical therapy, not a replacement.
Screen for undiagnosed malignancies before starting angiogenesis-promoting peptides, and monitor for side effects like injection-site reactions, kidney issues, or emotional numbness.
| Peptide | Primary Mechanism (2026 Update) | Common Orthopedic Application |
|---|---|---|
| BPC-157 | FBXO22-BACH1 axis; VEGFR2 upregulation | Tendon-to-bone healing, Achilles repair |
| TB-500 | Cell migration; anti-inflammatory pathways | Muscle repair, fracture healing |
| GHK-Cu | ECM remodeling; wound healing | Skin and soft tissue repair |
Neurocognitive and Mood-Modulating Peptides: Brain Health Advances
Peptides like Semax, Selank, and Cerebrolysin have drawn increased attention in 2026, thanks to new trial data and potential regulatory changes that could expand their availability through compounding pharmacies.
Key 2025–2026 Research Findings
In February 2026, the Department of Health and Human Services (HHS) announced plans to reclassify Semax and Selank from FDA Category 2 to Category 1. This reclassification, pending a Pharmacy Compounding Advisory Committee (PCAC) review on July 24, 2026, would allow licensed compounding pharmacies to dispense these peptides with a valid prescription.
On the clinical trial front, P21 has shown promising results. A 2025 Phase 2b trial revealed that P21 (administered at 5 mg/day subcutaneously for 28 days) reduced post-concussive symptom severity by 34% at 90 days in traumatic brain injury (TBI) patients, compared to 12% for placebo. Another Phase 2b study reported a 23% reduction in tau protein accumulation over 24 weeks in patients with early-stage cognitive decline. Additionally, Cerebrolysin demonstrated a 3.2-point improvement on the ADAS-Cog scale in a 500-patient Phase 3 vascular dementia trial, compared to 0.8 points for placebo. However, it has not yet shown measurable benefits in functional independence or daily living activities.
Mechanistically, Semax functions as a synthetic ACTH(4-10) analog, influencing dopaminergic and serotonergic systems. Selank, a synthetic tuftsin analog, exerts anxiolytic effects through GABAergic modulation, without the sedation or dependency risks linked to benzodiazepines. Russian trials have shown Selank can reduce anxiety scores by approximately 70%, without impairing cognitive function.
"The midlife brain is not having a feelings problem, it is going through a massive and measurable biological transition, with shifts in neuroplasticity, neurotransmitters, and neurotrophic signaling." - Sara Szal, MD
Among newer compounds, Dihexa stands out for its potency - reported to be 10 million times stronger than BDNF in promoting synaptogenesis in preclinical models. However, it lacks Phase 2 human data, and animal studies have flagged elevated liver enzymes at high doses.
These findings highlight the importance of precise dosing and monitoring protocols.
Clinical Dosing and Monitoring
Recent research has informed practical dosing strategies for neurocognitive peptides. Intranasal delivery is the preferred method for Semax and Selank, as it bypasses the blood-brain barrier via the olfactory mucosa while limiting systemic exposure. The modified version, NA-Semax-Amidate, has gained popularity in 2026 due to enhanced resistance to enzymatic breakdown and a longer half-life. Its primary mechanism involves BDNF upregulation via TrkB receptors in the hippocampus and frontal cortex.
Typical dosing for Semax ranges from 200–600 mcg/day, while Selank is administered at 100–300 mcg, one to three times daily. To prevent receptor downregulation, many clinicians recommend cycling these peptides - using them for 10–14 days followed by a 10-day break. A combined approach, pairing Selank for anxiety and hyperarousal with Semax for BDNF deficiency and motivation issues, is gaining traction as a dual strategy for mood and cognitive challenges.
"A peptide without a psychiatric evaluation is a mechanism searching for a target." - Dr. Shantanu Baghel, Psychiatrist
Before starting treatment, clinicians should rule out reversible causes of cognitive symptoms, such as sleep apnea, thyroid problems, B12 deficiency, and anemia. Monitoring for side effects like nasal irritation, headaches, dizziness, and blood pressure changes is also essential.
Risk-Benefit Analysis
Careful consideration of risks and benefits is crucial when incorporating these peptides into clinical practice. As of early 2026, only P21 and Cerebrolysin have published Phase 2 or Phase 3 human efficacy data. A 2024 meta-analysis revealed that fewer than 8 out of 47 marketed cognitive peptides had any published human clinical evidence, reflecting the uneven progress in this field.
Cerebrolysin has shown potential safety concerns at very high doses, with a Cochrane-style review indicating a higher risk of non-fatal serious adverse events (relative risk 2.15). For Semax, sustained BDNF elevation poses a theoretical risk; a 2025 study in rodents linked prolonged BDNF elevation to impaired memory consolidation, reinforcing the need for cycling protocols.
"Selank appears to modulate GABAergic tone more selectively, reducing anxiety without the global suppression that makes benzodiazepines problematic for long-term use." - Dr. Shantanu Baghel
This analysis helps guide clinicians in safely integrating these peptides into treatment plans.
| Peptide | Primary Target | Mechanism | Clinical Evidence Level |
|---|---|---|---|
| Semax | Cognition, mood | BDNF upregulation; dopamine/serotonin modulation | Russian clinical trials; FDA review 2026 |
| Selank | Anxiety, PTSD | GABAergic modulation; enkephalin degradation inhibition | Russian RCT data; ~70% anxiety score reduction |
| Cerebrolysin | Neurodegeneration | Multi-peptide neurotrophic support | Phase 3 completed; ADAS-Cog improvement confirmed |
| P21 | TBI, cognitive decline | CNTF derivative; BDNF/NGF upregulation | Phase 2b completed; 34% TBI symptom reduction |
Sourcing high-quality peptides remains critical. By 2026, the standard for research-grade neurocognitive peptides requires ≥98% purity verified by HPLC, with endotoxin levels below 0.5 EU/mg. Clinicians should always request batch-specific certificates to ensure safety and efficacy before prescribing.
Dermatologic and Aesthetic Peptides: Skin, Hair, and Anti-Aging Therapies
The field of peptides in dermatology and aesthetics has grown significantly as we approach 2026. Thanks to more robust clinical data, practitioners now have clear guidance when designing skin and anti-aging treatment plans. These therapies have advanced through rigorous studies, building on research in areas like metabolism, regeneration, and neurocognition. As a result, dermatologic peptides now provide reliable solutions for tackling skin and aging-related concerns.
2025–2026 Evidence Highlights
A 2026 meta-analysis of 19 randomized controlled trials (RCTs) involving 1,341 participants revealed that oral polypeptides outperform topical options for improving skin hydration (MD: 5.80, p < 0.01) and reducing wrinkles (MD: 0.35, p = 0.05). Topical formulations showed only modest effects on wrinkle reduction (MD = 0.27), largely because peptides struggle to penetrate the skin's outer barrier, the stratum corneum. Notably, only two of the 19 trials focused on topical delivery.
Among oral options, Bioactive Collagen Peptides (BCP) stood out. A daily dose of 10 g over 12 weeks significantly reduced both the number (p < 0.0002) and length (p < 0.0424) of facial wrinkles in middle-aged women. Peptpure® BCP, specifically, demonstrated broader benefits by increasing systemic levels of Klotho and TGF-β, markers linked to regenerative and anti-aging pathways.
"A 12-week course of Peptpure® BCP supplementation improved facial skin health, underlined by increased systemic levels of TGF-β and Klotho, suggesting activation of regenerative and antiaging pathways." - Dermatology and Therapy
Another standout, GHK-Cu, is a copper tripeptide with impressive scientific backing. Plasma levels of GHK-Cu drop by about 60% between ages 20 and 60, correlating with declines in skin density and repair capacity. Research shows it affects around 31% of human genes, enhancing antioxidant defenses and DNA repair while reducing inflammation. For topical use, Argireline (Acetyl Hexapeptide-3) has proven effective in clinical trials, reducing periorbital wrinkle depth by up to 48.9%.
Safety Considerations in Aesthetic Practice
While most peptides in this category are considered safe, some precautions are necessary. Melanocortin agonists like Bremelanotide (PT-141) can cause side effects such as nausea and temporary hypertension. Additionally, these peptides require strict UV protection due to photosensitivity risks, which are well-documented in U.S. dermatologic practice. Melanotan II, in particular, has been linked to cases of melanoma and kidney dysfunction and remains unapproved.
Clinicians should ensure product purity by sourcing peptides from regulated pharmacies and checking batch-specific certificates. Growth hormone (GH) secretagogues like CJC-1295 and Ipamorelin, often used in anti-aging protocols, are not suitable for patients with a history of cancer due to their potential to promote tumor growth via IGF-1. Regular IGF-1 monitoring is essential when using these peptides.
By addressing these safety concerns, practitioners can confidently incorporate peptides into aesthetic treatments.
Integrating Peptides into Aesthetic Protocols
To maximize results, consider a multimodal approach that combines oral collagen peptides for overall hydration with topical signal peptides for targeted wrinkle reduction. Start with 10 g/day of oral BCP for at least 12 weeks as a foundation, then add topical GHK-Cu or Argireline for specific concerns.
For enhanced effects, peptides like GHK-Cu can be paired with lasers or fillers to boost fibroblast activity and extracellular matrix (ECM) synthesis, improving recovery and outcomes. When choosing topical formulations, opt for products featuring carrier peptides or fatty acid attachments (e.g., palmitoyl pentapeptide) to improve skin penetration. Here's a summary of evidence grades for commonly used aesthetic peptides:
| Peptide | Administration | Primary Benefit | Evidence Grade |
|---|---|---|---|
| GHK-Cu | Topical / Injectable | Collagen synthesis, skin density | B |
| Argireline | Topical | Dynamic wrinkle reduction | B |
| Oral BCP | Oral | Systemic hydration, elasticity | B |
| Ipamorelin | Injectable | Lean mass, skin thickness | B/C |
| Epitalon | Injectable (cycled) | Telomere/pineal support | C |
Before initiating GH secretagogue-based treatments, conduct baseline tests, including IGF-1, CRP, and a comprehensive metabolic panel, to screen for contraindications and establish a monitoring framework.
Immunomodulatory Peptides: Applications in Inflammatory and Autoimmune Disorders
Peptide therapies targeting the immune system have made significant progress, reaching a new level of clinical development by 2026. These therapies are now competing with injectable biologics in treating conditions like psoriasis, rheumatoid arthritis (RA), and inflammatory bowel disease (IBD). In some cases, they even offer similar results in a convenient oral format.
Recent Advances in Clinical Research
One standout development is Icotrokinra (JNJ-77242113), an oral IL-23 receptor antagonist that has shown impressive results in achieving skin clearance. During the Phase 3 ICONIC-ADVANCE 1 & 2 trials, which included 1,505 adults, a daily dose of 200 mg led to 68–70% of patients achieving IGA 0/1 (clear or almost clear skin) by week 16. By week 24, 65–66% of patients reached PASI 90, compared to 41–43% for the TYK2 inhibitor deucravacitinib. Placebo responses were much lower, at just 9–11% for IGA 0/1.
"Icotrokinra is the first oral IL-23R antagonist to achieve high and durable levels of skin clearance with a favorable safety profile... overcoming key limitations of oral small molecules." - American Journal of Clinical Dermatology
In the field of RA, Peptide P01, discovered through AI, is an IL-6 receptor antagonist with an IC50 of approximately 1.6 µM. It effectively blocks IL-6/IL-6R binding and reduces STAT3 signaling without causing cytotoxic effects. Meanwhile, research led by Professor Helen McGettrick at the University of Birmingham showcased the potential of synthetic PEPITEM, a 14–amino-acid peptide. In animal models of inflammatory arthritis, PEPITEM reversed joint swelling to a degree comparable to infliximab and significantly increased Foxp3 transcripts, which are linked to immune suppression.
"There could be significant benefits over existing therapies, which are immunosuppressive in otherwise healthy populations, the risk of toxicity from natural peptide is extremely low, and administration in early disease could reduce reliance on steroids." - Professor Helen McGettrick, University of Birmingham
These breakthroughs point toward more personalized treatment options and opportunities to combine these peptides with existing therapies.
Patient Selection and Monitoring
Icotrokinra is particularly well-suited for patients with moderate-to-severe plaque psoriasis or IBD who prefer oral treatments, have a fear of needles, or have not responded to standard oral systemic therapies. For RA patients who do not respond to TNF inhibitors or DMARDs, peptides like P01 and PEPITEM provide early-intervention alternatives with reduced risks of broad immunosuppression.
A key advantage of oral peptides is their metabolism. Most are broken down by peptidases rather than CYP450 enzymes, greatly lowering the risk of liver-related drug interactions. However, patient monitoring remains essential. For example, in icotrokinra trials, mild infections such as nasopharyngitis and upper respiratory infections were the most common side effects, occurring at rates similar to placebo. No dose-dependent toxicity was observed. Patients with active or recent malignancies should avoid peptides that work through growth-factor mechanisms.
Integration with Standard Therapies
Immunomodulatory peptides are being integrated into treatment regimens as complementary options rather than outright replacements. For instance, Thymosin alpha-1 (Tα1) helps restore cellular immunity by activating TLR9 and boosting Th1 cytokines like IL-2 and IFN-γ. This makes it useful for immunosuppressed patients and as a vaccine adjuvant. Similarly, KPV (Lys-Pro-Val), a tripeptide derived from α-MSH, is being added to IBD protocols to suppress NF-κB signaling and reduce pro-inflammatory cytokines. KPV is currently under PCAC review, with a decision expected on July 23, 2026.
The table below provides a snapshot of the clinical progress for key immunomodulatory peptides:
| Peptide | Target/Mechanism | Primary Indication | Clinical Stage |
|---|---|---|---|
| Icotrokinra | IL-23R Antagonist | Psoriasis, IBD | Phase 3 |
| Peptide P01 | IL-6R Antagonist | Rheumatoid Arthritis | Preclinical |
| PEPITEM | Adiponectin-PEPITEM Pathway | Inflammatory Arthritis | Preclinical |
| Thymosin α1 | TLR9 / Th1 Cytokines | Immunodeficiency, Viral Infections | Clinical Use |
| KPV | NF-κB / α-MSH Derivative | IBD, Inflammation | PCAC Review July 2026 |
To ensure safety, peptides should be sourced from 503A-licensed pharmacies with verified batch certification. A 2018 study revealed that some research-grade peptides had purity levels as low as 5–75%, with certain samples containing lead concentrations exceeding safety limits by tenfold. These advancements in immunomodulatory peptides are expanding the options available for targeted immune interventions, complementing a wide range of existing therapies.
Regulatory and Safety Developments: What Clinicians Need to Know in 2026
The regulatory landscape for prescribing peptides is shifting in 2026, with new FDA actions that clinicians must adapt to. These changes directly impact how peptides can be accessed and prescribed, making it essential for healthcare professionals to stay informed.
Key FDA Announcements and Enforcement Actions

On April 15, 2026, the FDA removed 12 peptides from the "Bulk Drug Substances that Raise Significant Safety Concerns" (Category 2) list, effective April 22, 2026. This includes substances like BPC-157, TB-500, Melanotan II, and KPV. However, this removal does not mean these peptides are now approved for compounding.
"Removal from Category 2 does not equal Category 1 approval. Peptides removed from Category 2 remain in a regulatory limbo as unapproved new drugs." - Yoon Hang Kim, MD, MPH
These peptides remain unapproved for compounding under Section 503A, pending further FDA decisions. Seven peptides, including BPC-157, TB-500, and MOTs-C, are scheduled for PCAC review on July 23–24, 2026. If approved, they could move into Category 1, making them legally compoundable. The remaining five, such as GHK-Cu (injectable) and LL-37, are set for review in February 2027.
Separately, on May 1, 2026, the FDA proposed removing semaglutide, tirzepatide, and liraglutide from the 503B bulks list. This would effectively end large-scale compounding of these GLP-1 medications, as commercial shortages have eased. The FDA's reasoning hinges on its updated "clinical need" standard: if an FDA-approved drug adequately serves the patient population, compounding options will be restricted. These enforcement measures have led professional organizations to release updated guidance.
Professional Guidelines and Consensus Statements
Professional bodies have responded to these regulatory updates with new guidelines. In May 2026, ECRI and ISMP published a joint white paper highlighting the rapid growth of the commercial compounded peptide market, which has outpaced clinical research. For instance, they noted that 35 of 36 published studies on BPC-157 were conducted in animals, with no Phase 1 human safety data available.
"The commercial market for these compounded peptides has grown far faster than the science. Patients are injecting substances that have never been adequately tested in humans." - Rita Jew, PharmD, MBA, BCPPS, President of ISMP
In April 2026, an evidence-based grading framework (Levels A–D) was introduced to help clinicians evaluate peptides using comprehensive clinical monographs based on research quality. Level A represents robust evidence from large RCTs, while Level D includes peptides supported only by mechanistic hypotheses. Most compounded peptides currently fall into Level C or D, emphasizing the need for caution and informed consent when prescribing.
Reducing Risk in Clinical Practice
Clinicians can take several steps to minimize compliance risks and ensure patient safety:
- Audit pharmacy partners: Work exclusively with 503A-licensed pharmacies that source pharmaceutical-grade ingredients from FDA-registered facilities. RUO (Research Use Only) labels do not protect against legal risks.
- Document clinical rationale: When prescribing compounded peptides with FDA-approved analogs, clearly document why the approved product does not meet the patient's needs.
- Stay updated on regulatory reviews: Monitor Docket FDA-2025-N-6895 for outcomes from the July 2026 PCAC meeting. Positive recommendations could alter the legal status of several key peptides.
Adverse event reporting is equally critical. A survey of 508 patients using peptides revealed that 19% experienced side effects, though serious adverse events were rare (under 1%). Establishing protocols for tracking and reporting issues like immune reactions or injection-site problems is vital for patient safety and regulatory compliance. By implementing these measures, clinicians can navigate the evolving regulatory environment with greater confidence and care.
Conclusion: Applying 2026 Peptide Research in Clinical Practice
Key Takeaways for Clinicians
The year 2026 brought significant progress in peptide research. For instance, triple receptor agonists like retatrutide demonstrated a mean body weight reduction of 24.7% over 28 weeks - approximately 40% greater than the tirzepatide Phase 3 results. Advances in delivery methods also stood out, with intranasal delivery using chitosan-based carriers achieving central nervous system (CNS) bioavailability rates of 18–22% for neuroprotective peptides. Meanwhile, in aesthetic medicine, a meta-analysis of 19 randomized controlled trials confirmed that oral polypeptides outperform topical formulations for improving skin hydration and reducing wrinkles. Alongside these breakthroughs, the regulatory environment continues to evolve, requiring close attention from clinicians.
The regulatory landscape remains uncertain. Upcoming PCAC reviews in July 2026 will play a critical role in determining which peptides U.S. clinicians can legally compound and prescribe. Until those decisions are finalized, some peptides exist in a regulatory gray area, raising potential legal concerns.
"The big picture is that peptides are a legitimate, powerful class of therapeutics, but the legitimacy is confined to a relatively narrow subset of them." - Peter Attia, MD
To ensure safety in clinical practice, two key principles should guide clinicians: apply the A–D evidence framework and screen for active malignancy before prescribing any regenerative peptide with angiogenic properties.
Using PeptidePrescriber for Evidence-Based Practice
Given the rapid pace of developments - marked by over 470 active peptide research programs worldwide - staying updated across metabolic, regenerative, neurocognitive, aesthetic, and immunomodulatory applications is crucial. PeptidePrescriber is a valuable resource for clinicians navigating this fast-changing field. The platform provides access to 2026-updated monographs, dosing calculators, and regulatory trackers, all tailored to the needs of licensed professionals.
Its tools are especially helpful for managing the transition from dual to triple agonist protocols, where precision in titration is critical. Features like reconstitution and unit conversion calculators help reduce dosing errors in complex treatment regimens. Additionally, the platform’s regulatory reference library keeps clinicians informed about the shifting 503A/503B compounding rules. For those working with off-label or compounded peptides, informed consent templates and implementation checklists offer practical support for maintaining compliance.
FAQs
Which peptides in 2026 have the strongest human trial evidence?
By 2026, peptides with the most robust human trial evidence are those that have successfully passed Phase III trials and received regulatory approval. Here's a look at some of the standout performers:
- Semaglutide and tirzepatide: These peptides are at the forefront of weight management and metabolic health, showing impressive results in helping individuals manage weight effectively.
- Retatrutide: This peptide has delivered encouraging outcomes in weight loss studies, making it a strong contender in the field.
- Icotrokinra: Known for its lasting impact on skin clearance, this peptide has proven effective in treating plaque psoriasis.
- Myoki: This peptide has demonstrated its ability to enhance muscle mass and strength, offering hope for patients dealing with muscle atrophy.
These advancements highlight the growing potential of peptides in addressing diverse health challenges.
How do 2026 FDA compounding changes affect what I can prescribe?
As of May 2026, the FDA has not approved the routine compounding of the 12 peptides that were recently taken off the Category 2 "Do Not Compound" list. These peptides are still in a regulatory gray area and cannot currently be legally compounded under Section 503A. The Pharmacy Compounding Advisory Committee is set to review seven of these peptides on July 23-24, 2026. Keep an eye on FDA updates for more information.
What safety screening should I do before using regenerative peptides?
Before starting regenerative peptides, it's essential to conduct a detailed clinical evaluation to identify any potential risks. Screening for undiagnosed cancer is particularly important since many peptides encourage angiogenesis, which could carry certain risks. Take a close look at the patient’s health history, including their medications, lab results, hormone levels, and stress factors. Make sure the treatment is based on a well-understood mechanism of action, has demonstrated effectiveness, presents a clear risk-benefit balance, and comes from regulated, FDA-registered compounding pharmacies.