
Peptide therapy is becoming a regulated yet popular treatment option for managing hormones, tissue repair, and metabolism. However, prescribing peptides comes with strict rules and responsibilities, especially with recent FDA changes in 2026. Here's what you need to know:
- FDA-Approved vs. Compounded Peptides: FDA-approved peptides (e.g., Semaglutide, PT-141) are backed by clinical trials and can be prescribed off-label, while compounded peptides (e.g., BPC-157, TB-500) face stricter regulations, limited safety data, and higher legal risks.
- Regulatory Updates: As of 2026, 19 commonly used peptides, including BPC-157 and CJC-1295, are reclassified as "Category 2" and cannot be compounded due to safety concerns.
- Patient Evaluation: Proper diagnosis, contraindication checks, and baseline labs (e.g., IGF-1, HbA1c) are essential before prescribing.
- Sourcing Compliance: Only use licensed 503A or 503B pharmacies, verify Certificates of Analysis (CoA), and avoid research-grade peptides labeled "for research use only."
- Dosing Protocols: Start with low doses and titrate slowly while monitoring for side effects like nausea (GLP-1 agonists) or insulin resistance (GH secretagogues).
- Monitoring: Regular follow-ups (every 6–8 weeks initially) and lab tests are critical to track therapy safety and effectiveness.
Peptide therapy requires thorough documentation, informed consent, and compliance with evolving regulations to protect both patients and your practice. Always prioritize patient safety and legal adherence when incorporating peptides into your clinical workflow.
Peptide Therapy Prescribing Checklist: Key Requirements by Peptide Class
Peptide & Hormone Therapies for Health, Performance & Longevity | Dr. Craig Koniver
sbb-itb-7164bd9
Patient Evaluation and Eligibility Checklist
Not every patient who inquires about peptide therapy will be a suitable candidate. A structured evaluation process is key to ensuring patient safety and maintaining compliance, starting well before a prescription is written.
Define the Indication and Clinical Goals
First, clarify why the peptide is being considered for this patient. Document a specific chief complaint that justifies its use, particularly when conventional treatments have proven insufficient. Avoid vague objectives like "feeling better" or "anti-aging." Instead, focus on clear, measurable goals - such as aiding tissue repair after an injury, improving metabolic function in pre-diabetes, or managing immune deficiencies with documented evidence.
Additionally, determine whether the peptide is FDA-approved or compounded. Each type comes with unique evidence requirements, legal considerations, and informed consent protocols.
Once these goals are established, move on to a detailed review of the patient’s medical history.
Review Medical History and Contraindications
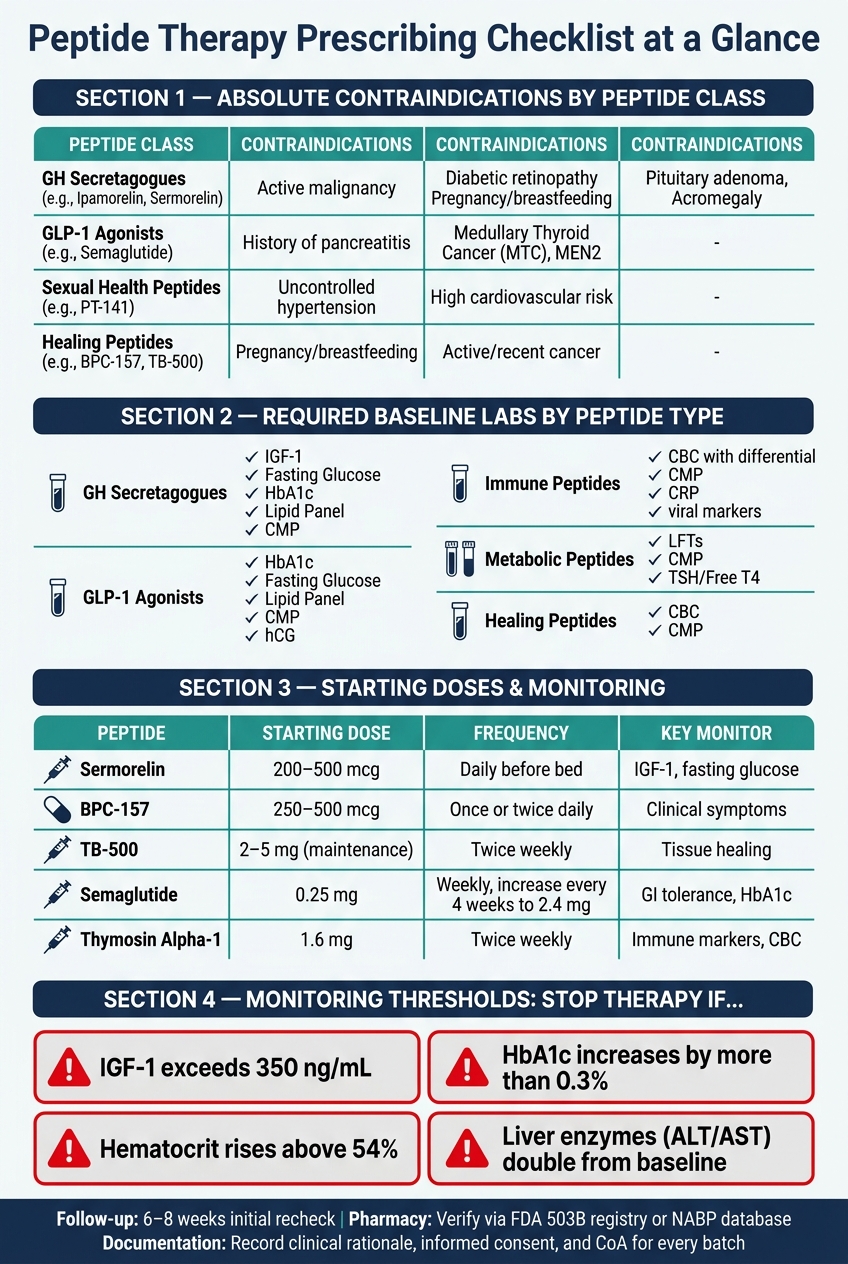
With the goals defined, the next step is to assess the patient’s medical history for factors that could affect the safety or effectiveness of the peptide. Contraindications vary widely depending on the peptide class, so a generic intake form won’t suffice. The table below outlines key absolute contraindications for common peptide categories:
| Peptide Class | Absolute Contraindications |
|---|---|
| GH Secretagogues (e.g., Ipamorelin, Sermorelin) | Active malignancy, diabetic retinopathy, pregnancy/breastfeeding, pituitary adenoma, acromegaly |
| GLP-1 Agonists (e.g., Semaglutide) | History of pancreatitis, Medullary Thyroid Cancer (MTC), Multiple Endocrine Neoplasia type 2 (MEN2) |
| Sexual Health Peptides (e.g., PT-141) | Uncontrolled hypertension, high cardiovascular risk |
| Healing Peptides (e.g., BPC-157, TB-500) | Pregnancy/breastfeeding, active or recent cancer (due to theoretical angiogenesis risks) |
After identifying contraindications, perform medication reconciliation. Adjust treatments such as diabetes medications and monitor therapies involving thyroid hormones, anticoagulants, corticosteroids, or oral hypoglycemics as necessary.
Once the history review is complete, proceed to order baseline labs.
Order Baseline Labs and Diagnostic Tests
Baseline labs are critical to understanding the patient’s starting health status. The specific tests depend on the peptide being considered, but the guiding principle is simple: never prescribe without knowing the patient’s baseline.
"Lab monitoring is not optional for GH secretagogue protocols - IGF-1, fasting glucose, and a metabolic panel before starting... are the minimum standard." - Dr. James Okafor, PharmD, Clinical Reviewer
| Peptide Type | Required Baseline Tests |
|---|---|
| GH Secretagogues | IGF-1, Fasting Glucose, HbA1c, Lipid Panel, CMP |
| GLP-1 Agonists | HbA1c, Fasting Glucose, Lipid Panel, CMP, Pregnancy Test (hCG) |
| Immune Peptides | CBC with differential, CMP, CRP, relevant viral markers |
| Metabolic Peptides | LFTs, CMP, TSH/Free T4 |
| Healing Peptides | CBC, CMP (if systemic conditions exist) |
For patients of childbearing potential, a urine or serum hCG test is mandatory before starting most peptide therapies. If prescribing PT-141, check blood pressure at baseline due to its potential to cause temporary increases. Plan to repeat the full panel of tests in 8–12 weeks to evaluate the therapy’s impact.
Regulatory, Legal, and Sourcing Compliance
After completing patient evaluations and baseline lab work, the next step is ensuring compliance with regulatory and sourcing requirements. Peptide therapy operates in a highly regulated environment, and since 2024, these rules have become stricter. Any misstep here can lead to serious consequences, including license suspension or even clinic closure.
Confirm the Regulatory Status of Each Peptide
Before prescribing, it's essential to verify the FDA regulatory status of each peptide. A few peptides, such as Sermorelin, Bremelanotide (PT-141), Oxytocin, and Tesamorelin, are FDA-approved and can be prescribed off-label through standard pharmacies based on clinical judgment. For other peptides, additional scrutiny is required.
Since 2026, many wellness peptides have been reclassified as Category 2, meaning they are considered to have "significant safety concerns" and cannot be compounded for human use. Additionally, with the GLP-1 shortage resolved in 2024–2025, the previous allowance for compounded semaglutide and tirzepatide has ended. Now, compounding these peptides is only allowed with documented, individualized medical necessity, such as a proven allergy to an inactive ingredient in a commercial product.
It's also important to note that labels like "Research Use Only" (RUO) offer no legal protection in clinical settings. Regulators evaluate the full clinical context, not just the label.
"Legal compounding channels for these peptides have been effectively closed. If a licensed 503A pharmacy cannot legally compound them, any clinic obtaining these substances is almost certainly sourcing from research-chemical suppliers." - Yoon Hang "John" Kim, MD, MPH
Choose a Reputable Pharmacy and Verify Sourcing Standards
Once you've confirmed that a peptide can legally be compounded, the next step is selecting a reliable pharmacy. Understanding the two types of pharmacies is critical:
- 503A pharmacies: Regulated by state boards, these pharmacies require individual patient prescriptions for every order.
- 503B outsourcing facilities: Registered with the FDA, these facilities follow current Good Manufacturing Practice (cGMP) standards and can provide peptides for office use without patient-specific prescriptions.
To confirm a pharmacy's credentials, use the FDA's Outsourcing Facility database to verify 503B registration and the NABP Drug Outlet Verification database to check state licensure for 503A pharmacies. Always request a batch-specific Certificate of Analysis (CoA) that confirms identity (via mass spectrometry) and purity (≥98% by HPLC). Ensure the CoA's lot number matches the one on the vial. Additional quality indicators include accreditation from organizations like PCAB (Pharmacy Compounding Accreditation Board) or ACHC. Be cautious of unusually low prices, as they may signal issues with sterility or potency. If a pharmacy refuses to provide third-party CoAs, avoid prescribing from them.
The risks of non-compliance are serious. For example, in 2024–2025, the Ohio Board of Pharmacy suspended clinics simply for possessing research-labeled vials of AOD-9604, BPC-157, and Ipamorelin - even when no patient harm occurred. Ensuring compliant sourcing is essential before moving on to dosing and patient management.
Maintain Proper Compliance Documentation
Thorough documentation is your best legal safeguard. Always record a clear clinical rationale for using a compounded peptide, along with detailed informed consent that explains the peptide's non–FDA-approved status and any limitations in clinical evidence. Importantly, document the actual conversation with the patient in your clinical notes - relying solely on a signed form is not enough to prove the patient made an informed decision.
Keep records of the pharmacy's licensure, any PCAB or ACHC accreditation, and CoAs for each batch dispensed to patients. For telehealth providers, document an active license in the patient's state and confirm that the pharmacy is licensed to ship there. Be aware that standard malpractice policies often exclude coverage for unapproved drugs, which means clinicians prescribing Category 2 peptides could face personal liability if adverse events occur. Detailed, contemporaneous records are key to showing that clinical decisions were medically justified.
These compliance steps form the backbone of safe and lawful peptide therapy, building on the patient evaluation protocols discussed earlier.
Dosing, Administration, and Patient Education
Establishing a safe and effective dosing protocol is key. It’s not just about getting the dose right - it’s also about ensuring patients can administer it properly.
Set Starting Doses and Titration Schedules
The mantra here is "start low, go slow." Beginning with the lowest dose in the therapeutic range allows you to see how a patient tolerates the peptide before increasing the dose. Since many side effects are dose-dependent, this cautious approach helps minimize risks.
Doses should be tailored to the patient based on factors like age, kidney function, and current medications. For example, with growth hormone secretagogues like Sermorelin or Ipamorelin, starting doses should be guided by baseline IGF-1, fasting glucose, and HbA1c levels. For GLP-1 receptor agonists like semaglutide, the recommended starting dose is 0.25 mg weekly, gradually increasing every 4 weeks to a target of 2.4 mg. This slower titration schedule helps reduce nausea, a common side effect reported by 20–44% of patients during the adjustment period.
Here’s a quick summary of starting doses and titration protocols for various peptides:
| Peptide | Starting Dose | Titration / Frequency | Key Monitoring Factor |
|---|---|---|---|
| Sermorelin | 200–500 mcg | Daily before bed | IGF-1, fasting glucose |
| BPC-157 | 250–500 mcg | Once or twice daily; 6–12 week cycles | Clinical symptom tracking |
| TB-500 | 2–5 mg (maintenance) | Twice weekly (loading: 5–10 mg) | Tissue healing progress |
| Semaglutide | 0.25 mg | Weekly; increase every 4 weeks to 2.4 mg | GI tolerance, HbA1c, weight |
| Thymosin Alpha-1 | 1.6 mg | Twice weekly | Immune markers, CBC |
Timing also matters. For instance, growth hormone secretagogues should be taken before bed to align with the body's natural nighttime GH pulse. Additionally, most protocols recommend cycling - typically 8–12 weeks on, followed by 4 weeks off - to avoid receptor desensitization or prolonged hormone elevation.
"Protocols that start at the low end of the dose range and titrate upward based on response and tolerance tend to produce fewer adverse events than loading protocols." - PeptaHub Safety Guide
When calculating injection volumes, use this formula: Dose (mcg) ÷ Concentration (mcg/mL). On a U-100 syringe, 1 unit equals 0.01 mL.
Once dosing is set, it’s time to ensure patients are confident in administering their therapy.
Teach Patients How to Administer Peptides
Most peptides are delivered via subcutaneous injection, which provides nearly complete bioavailability. Patients will need a 28–31 gauge insulin needle (5/16 to 1/2 inch) and clear, step-by-step guidance for their first self-injection.
Reconstitution is a common trouble spot. Multi-dose vials should be reconstituted with bacteriostatic water (containing 0.9% benzyl alcohol) rather than sterile water, which is for single-use only. Patients should inject the water slowly down the side of the vial and gently swirl - shaking is a big no-no.
"Improper injection technique and reconstitution errors are the most preventable sources of harm in peptide therapy." - Dr. James Okafor, PharmD
Here are the key steps to teach:
- Wash hands thoroughly for at least 20 seconds.
- Swab the vial stopper and injection site with 70% isopropyl alcohol.
- Always use a new needle for each injection.
- Rotate injection sites (lower abdomen, lateral thighs, or flanks) to avoid lipohypertrophy.
- Store reconstituted vials in the refrigerator (36–46°F), not in the door where temperatures vary, and use within 28–30 days.
Patients should also know to discard any solution that appears cloudy, discolored, or contains particles. Never freeze vials - freezing can crack the vial or damage the peptide. Used needles should go straight into a sharps container to prevent accidental injury; recapping is not allowed.
For extra support, tools like PeptidePrescriber's injection site guide and reconstitution calculator can help patients and clinicians prepare for the first dose.
Once patients are comfortable with administration, they need to be prepared to monitor and manage side effects.
Identify and Manage Side Effects
Most side effects in peptide therapy are predictable and tied to dosage, so identifying them early is critical. Below is a breakdown of common side effects and serious warning signs by peptide class:
| Peptide Class | Common Side Effects | Serious Warning Signs |
|---|---|---|
| GLP-1 Agonists | Nausea, vomiting, diarrhea, constipation | Severe abdominal pain (pancreatitis), gallbladder pain |
| GH Secretagogues | Water retention, joint pain, signs of insulin resistance | Elevated blood glucose, carpal tunnel-like symptoms |
| Tissue Repair | Minor injection site redness and bruising | Expanding redness, warmth, pus, fever (infection) |
| Sexual Health (PT-141) | Flushing, nausea, transient blood pressure increases | Systemic allergic reactions, significant BP elevation |
For growth hormone secretagogues, watch for signs of insulin resistance, like excessive thirst or frequent urination, even if the patient feels fine. As Dr. James Okafor, PharmD, explains:
"The clinically relevant risks (insulin resistance, elevated IGF-1) do not produce noticeable symptoms until they are significant... the absence of symptoms does not confirm the absence of metabolic changes."
If side effects arise, adjust the dose or extend the dosing interval. For example, if a patient develops swelling in the ankles (peripheral edema) or tingling in the hands (paresthesia), a dose reduction or pause in therapy may be needed. Persistent numbness might indicate carpal tunnel-like symptoms, requiring further evaluation.
Injection site reactions like mild bruising or stinging are normal. However, spreading redness, warmth, or fever could signal cellulitis or an abscess, requiring immediate medical attention. Encourage patients to keep a symptom diary, noting daily doses, injection sites, and any reactions. This can reveal patterns during follow-up visits.
Finally, establish clear stopping criteria from the beginning. Therapy should be halted if there are signs of infection at the injection site, severe abdominal pain (especially with GLP-1 agonists), vision changes, or severe headaches.
Monitoring and Follow-Up Checklist
Once the appropriate dosing is set and patients are educated, the next step is consistent monitoring to ensure therapy is both safe and effective. After starting treatment, the focus shifts to keeping a close eye on patient progress. A well-structured monitoring plan is vital to ensure everything stays on course.
Set a Follow-Up Schedule
The first lab recheck should happen 6–8 weeks after starting therapy. This is a critical timeframe when markers like IGF-1 and early metabolic indicators stabilize.
"The 6 to 8 week draw is the most important one. That's when IGF-1 has stabilized on a new GH peptide dose, when hematocrit shifts are visible, and when any metabolic drift from MK-677 shows up." - Dr. James Walker, MD
After this initial check, follow-up frequency depends on the peptide being used. For example:
- GH secretagogues (e.g., Sermorelin, Ipamorelin): Recheck every 3 months.
- Metabolic peptides (e.g., semaglutide): Monitor every 4 to 8 weeks, especially while adjusting doses.
- Tissue repair peptides (e.g., BPC-157, TB-500): These are typically used in shorter cycles (6–12 weeks), so clinical reviews every 4 to 6 weeks are recommended.
Always confirm that patients are sourcing their peptides from a licensed 503A or 503B compounding pharmacy. This ensures quality and safety while setting a consistent schedule for clinical and lab evaluations.
Track Clinical and Lab Outcomes
Monitoring isn’t just about running tests - it’s about focusing on the right markers for each peptide class and responding to meaningful changes. Here’s an overview of key markers and follow-up timelines:
| Peptide Class | Key Monitoring Markers | Frequency |
|---|---|---|
| GH Secretagogues | IGF-1, Fasting Glucose, HbA1c | Every 3 months |
| GLP-1 Agonists | HbA1c, eGFR, BUN, Creatinine, TSH | Every 4–8 weeks |
| Tissue Repair Peptides | Clinical symptoms, CMP | Every 4–6 weeks |
| Immune Peptides | CBC with differential, hsCRP, CMP | Every 3–6 months |
Be vigilant about key thresholds. Stop therapy immediately if any of the following occur:
- IGF-1 exceeds 350 ng/mL
- HbA1c increases by more than 0.3%
- Hematocrit rises above 54%
- Liver enzymes (ALT/AST) double from baseline
These changes can happen without obvious symptoms, so regular lab checks are non-negotiable. Also, remind patients to stop taking biotin supplements at least 72 hours before blood draws. Biotin can interfere with lab results, particularly thyroid and hormone tests.
Assess and Report Adverse Events
Monitoring isn’t just about labs - it’s also about keeping an eye on clinical signs. At every visit, check injection sites for redness, swelling, warmth, or pain. Ask patients directly about symptoms like peripheral edema, joint stiffness, or tingling sensations, as they might not bring these up on their own. A symptom diary during the first 2 to 4 weeks can help establish a baseline.
Document everything: clinical decisions, patient responses, and any dose adjustments. For FDA-approved peptides, report any serious adverse events through the FDA MedWatch system. For compounded peptides, keep thorough internal records to protect both the patient and your practice.
"A provider who disappears after issuing a prescription is not providing clinical oversight. They are providing bureaucratic cover for a sale." - Meto Editorial Team
Consistent follow-up is what ensures peptide therapy stays on track. Prescribing is just the first step. Regular monitoring is where the real work begins.
Conclusion: Building a Safe Peptide Therapy Practice
Peptide therapy is advancing quickly, but it's happening alongside stricter regulatory oversight. For instance, the FDA has recently reclassified peptides like BPC-157, TB-500, and Ipamorelin into Category 2, which means they can no longer be compounded. On top of that, some states have started taking serious action, including freezing assets, suspending licenses, and pursuing civil settlements.
A well-organized checklist isn't just about better clinical practice - it’s also your first line of defense legally. Keeping thorough records of medical necessity, sourcing only from licensed pharmacies, and obtaining proper informed consent are critical steps to safeguard your license if regulators come calling. It’s also worth noting that standard malpractice policies often exclude claims involving unapproved drugs, so it’s crucial to confirm your coverage in writing. These legal safeguards form the backbone of a secure prescribing process.
"Innovative clinical thinking must always be paired with strict regulatory compliance." - Yoon Hang "John" Kim, MD, MPH
To build a safe and efficient practice, start small. Focus on 2–3 peptides that are well-researched and trusted. Verify the pharmacy through resources like the PCAB database or the FDA's 503B registry, and always request batch-specific Certificates of Analysis for added assurance. Streamlining your workflow with automated prescribing tools can save a lot of time - cutting the average prescription process from 25–35 minutes to just 3–5 minutes, a reduction of 85%. This means less time on paperwork and more time for patient care.
For additional support, tools like PeptidePrescriber provide a wealth of resources, including evidence-based dosing protocols, regulatory guidance, and clinical insights for safe prescribing. Public tools, such as a unit conversion calculator and injection site guide, are also available. The Starter Pack includes consent templates, a detailed implementation checklist, and a quick reference for regulatory compliance, making it easier to get your practice up and running. By grounding your prescribing decisions in thorough evaluations, compliant sourcing, and consistent monitoring, you can safeguard your patients and your practice effectively.
FAQs
How do I confirm a peptide is legal to prescribe and compound in 2026?
To ensure a peptide remains legal to prescribe and compound in 2026, follow these steps:
- Confirm the peptide is not included on the FDA's Category 2 restricted list for 503B outsourcing facilities.
- Verify that the peptide is obtained from a licensed 503A pharmacy or an FDA-registered 503B facility.
- Stay updated on FDA reviews, regulatory changes, and advisory committee evaluations.
Regularly monitoring these factors will help maintain compliance with evolving regulations.
What labs should I order before starting peptide therapy?
To ensure a safe starting point for peptide therapy, it's important to run the following tests:
- HbA1c and fasting glucose: These help evaluate blood sugar levels and detect any signs of diabetes or prediabetes.
- Comprehensive Metabolic Panel (CMP): Provides insight into kidney function, liver health, and overall metabolic status.
- Lipid panel: Assesses cholesterol levels and cardiovascular health.
- Complete Blood Count (CBC) with differential: Offers a snapshot of overall health, including immune function and potential infections.
- Thyroid screening: Includes TSH, free T4, and T3 (if necessary) to check for thyroid-related issues.
- Lipase: Recommended if there's any concern about pancreatitis.
- Pregnancy test: Essential for individuals who could be pregnant to ensure safety.
These tests establish a comprehensive baseline, helping to minimize risks and tailor the therapy to individual needs.
What are the top red flags to stop peptide therapy right away?
When it comes to peptide therapy, there are some warning signs you should never ignore. These include:
- Prescribing growth hormone peptides without checking baseline IGF-1 levels: IGF-1 is a critical marker for monitoring the effects of growth hormone peptides. Skipping this step can lead to unsafe or ineffective treatment.
- Using peptides from unverified sources: If a provider sources peptides from unreliable vendors instead of licensed pharmacies, it raises serious concerns about the quality and safety of the product.
- Lack of transparency about the compounding pharmacy: If your provider refuses to disclose or verify the compounding pharmacy or provide a Certificate of Analysis, that's a major red flag. This document is essential for confirming the purity and authenticity of the peptides.
To stay safe, always verify the source of your peptides and ensure proper protocols are followed. Trustworthy providers will prioritize transparency and your well-being.