Semaglutide and tirzepatide are two injectable treatments for type 2 diabetes and obesity, offering significant benefits in blood sugar control and weight loss. While both are effective, they differ in mechanisms, outcomes, and approved uses. Here's what you need to know:
- Semaglutide: A GLP-1 receptor agonist available as Ozempic (diabetes), Wegovy (weight management), and Rybelsus (oral tablet for diabetes). It reduces HbA1c by ~1% and supports long-term weight loss (~15% over 4 years). Approved for cardiovascular and kidney protection.
- Tirzepatide: A dual GIP/GLP-1 receptor agonist marketed as Mounjaro (diabetes) and Zepbound (weight management, sleep apnea). It achieves greater weight loss (~20-22%) and HbA1c reduction (~2.3%) but lacks long-term data beyond 72 weeks.
Quick Comparison
| Feature | Semaglutide (Wegovy/Ozempic) | Tirzepatide (Zepbound/Mounjaro) |
|---|---|---|
| Mechanism | GLP-1 receptor agonist | Dual GIP/GLP-1 receptor agonist |
| Avg. Weight Loss | ~15% | ~20-22% |
| HbA1c Reduction | ~1% | ~2.3% |
| FDA Approvals | Diabetes, obesity, CV, CKD | Diabetes, obesity, sleep apnea |
| Administration | Weekly injection or oral | Weekly injection only |
| Cost (Monthly) | $935-$1,349 | $1,060 (as low as $299 direct) |
Key Takeaway: Choose semaglutide for cardiovascular/kidney benefits or oral options. Opt for tirzepatide if maximum weight loss or aggressive glucose control is the goal. Both require careful titration to manage side effects like nausea and vomiting.
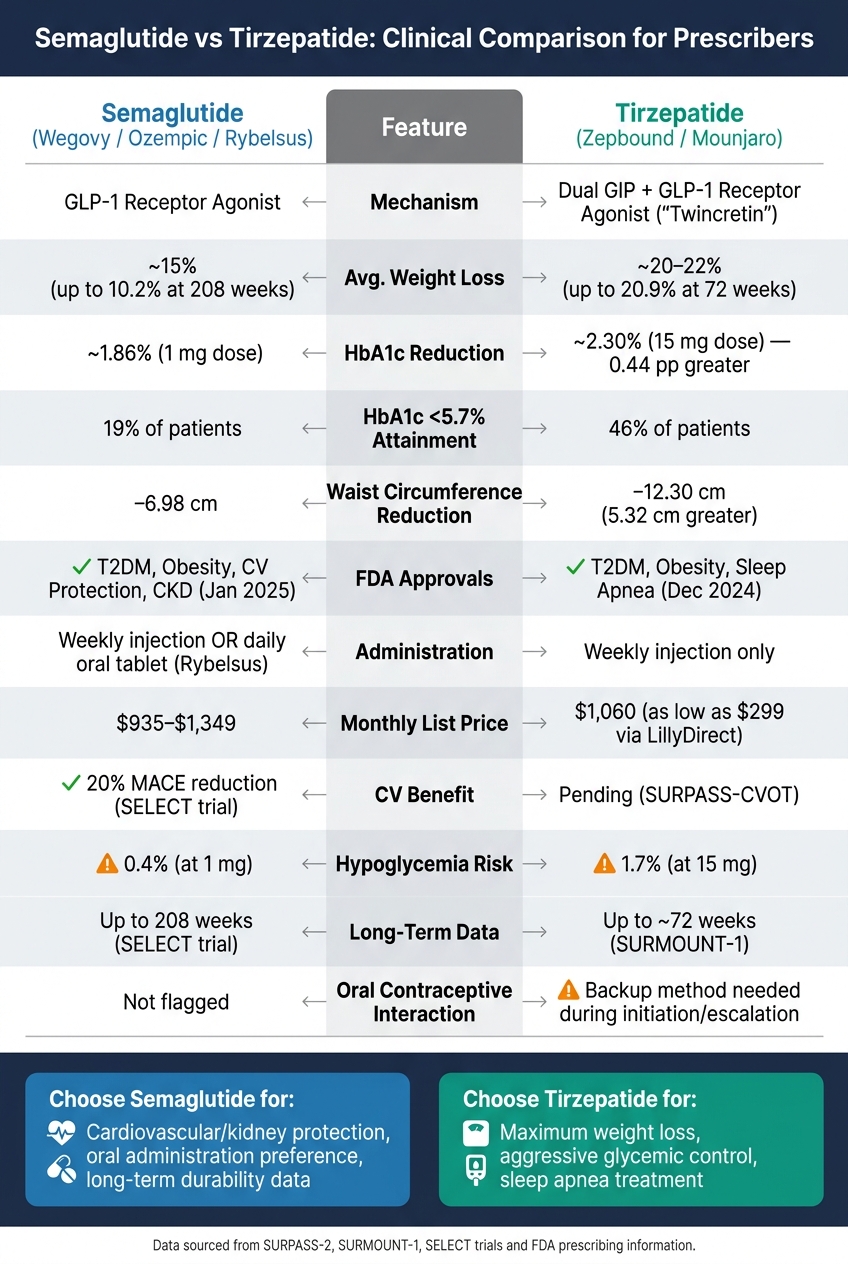
Semaglutide vs Tirzepatide: Clinical Comparison for Prescribers
Semaglutide: Mechanism, Uses, and Clinical Insights
Mechanism of Action
Semaglutide works as a GLP-1 receptor agonist, closely related to liraglutide and dulaglutide. It enhances glucose-dependent insulin secretion, reduces glucagon release, slows gastric emptying, and triggers feelings of fullness by acting on the hypothalamus. These combined effects help control blood sugar levels and promote satiety, which can aid in weight management.
The medication is broken down into amino acids by proteases in the body, with its effects lasting due to renal elimination. This extended action allows for once-weekly subcutaneous dosing, offering a more convenient alternative to daily injectables like liraglutide.
FDA-Approved Indications
Semaglutide's broad mechanism supports its approval for multiple conditions under three distinct brand names, each tailored to specific uses:
| Brand Name | Route | Primary FDA Indications |
|---|---|---|
| Ozempic | Subcutaneous | Managing type 2 diabetes (T2DM); reducing major adverse cardiovascular events (MACE) in T2DM with cardiovascular disease (CVD); lowering chronic kidney disease (CKD) risk in T2DM with CKD |
| Rybelsus | Oral | Managing T2DM; reducing MACE in T2DM with high cardiovascular risk |
| Wegovy | Subcutaneous | Long-term weight management (adults and children 12+); reducing MACE in overweight/obese individuals with CVD |
It's important to note: Wegovy should not be combined with Ozempic, Rybelsus, or any other GLP-1 receptor agonist. Additionally, Wegovy is approved for pediatric patients aged 12 and older who meet specific BMI criteria.
Dosing and Titration
Injectable semaglutide starts at 0.25 mg weekly, gradually increasing every four weeks to improve tolerability. For Ozempic, the maintenance dose ranges from 0.5 mg to 2 mg weekly, depending on blood sugar control. Wegovy, used for weight management, targets a maintenance dose of 2.4 mg weekly, though 1.7 mg is an option if the higher dose isn't well-tolerated.
For patients experiencing gastrointestinal side effects during titration, the dosing schedule can be adjusted by extending the current dose for an additional four weeks before increasing. This flexibility is particularly emphasized in Wegovy's prescribing guidelines.
For oral semaglutide (Rybelsus), proper administration is key. It must be taken on an empty stomach with no more than 4 ounces of plain water. Afterward, patients should wait at least 30 minutes before eating, drinking, or taking other medications.
Clinical Benefits and Limitations
Semaglutide has shown impressive results in clinical trials. In the SELECT trial, semaglutide 2.4 mg reduced major cardiovascular events by 20% in adults with obesity or overweight and established cardiovascular disease - regardless of diabetes status. Over four years, participants experienced an average weight loss of 10.2%, compared to just 1.5% with placebo. By week 104, 67.8% of participants achieved at least 5% weight loss. For type 2 diabetes, semaglutide typically lowers HbA1c by about 1% compared to control treatments.
However, its use isn't without challenges. Gastrointestinal side effects, especially nausea and vomiting during dose escalation, are common reasons for early discontinuation. Patients with diabetic retinopathy should be monitored closely, as rapid improvements in blood sugar can temporarily worsen the condition. Semaglutide is also contraindicated in individuals with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Clinicians should exercise caution when considering compounded semaglutide products, such as semaglutide sodium or semaglutide acetate. These are not equivalent to FDA-approved versions and have been linked to dosing errors and adverse events.
sbb-itb-7164bd9
Tirzepatide: Dual Mechanism and Clinical Applications
Mechanism of Action
Tirzepatide stands out by targeting two incretin pathways simultaneously, offering a different approach compared to semaglutide. While semaglutide focuses solely on the GLP-1 receptor, tirzepatide works as a dual agonist for both the GIP and GLP-1 receptors, earning it the nickname "twincretin." Its structure - a 39-amino acid peptide modeled after native GIP - includes a C20 fatty diacid moiety, which extends its half-life to about 5 days, allowing for convenient once-weekly dosing. Roughly 99% of tirzepatide binds to plasma albumin, contributing to its sustained action. It binds the GIP receptor with similar affinity to native GIP but has about one-fifth the GLP-1 receptor affinity of native GLP-1. However, its unique agonism, which favors cAMP signaling over β-arrestin recruitment, delivers strong metabolic effects. The GIP component is believed to enhance appetite suppression and improve insulin sensitivity, making tirzepatide versatile in its clinical applications.
FDA-Approved Indications
Tirzepatide is available under two brand names, each approved for specific uses:
| Brand Name | Primary FDA Indications |
|---|---|
| Mounjaro | Helps manage blood sugar in adults with type 2 diabetes, alongside diet and exercise |
| Zepbound | Aids in chronic weight management for adults with a BMI ≥30 kg/m², or BMI ≥27 kg/m² with at least one weight-related condition; also approved for moderate-to-severe obstructive sleep apnea in adults with obesity |
Patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use tirzepatide, similar to semaglutide.
Dosing and Titration
Tirzepatide starts at a low dose of 2.5 mg, administered subcutaneously once a week for the first 4 weeks. After this initial phase, the dose is increased in 2.5 mg increments every 4 weeks. Maintenance doses typically range from 5 mg to 15 mg, depending on how well the patient tolerates the medication and their response to it. If a weekly dose is missed, it can be taken within 4 days (96 hours). If more than 4 days have passed, the missed dose should be skipped, and the regular schedule resumed. For those using oral contraceptives, a non-oral or barrier method is recommended for 4 weeks after starting tirzepatide or after each dose increase.
Clinical Benefits and Limitations
Tirzepatide has shown impressive results in clinical trials. In the SURPASS-2 trial, patients taking the 15 mg dose saw HbA1c levels drop by 2.30 percentage points and experienced an average weight loss of 11.2 kg over 40 weeks. The SURMOUNT-1 trial, which focused on individuals without diabetes, revealed that the 15 mg dose led to an average body weight reduction of 20.9% over 72 weeks. Remarkably, 96.3% of participants on tirzepatide achieved at least a 5% weight loss, compared to just 27.9% in the placebo group.
However, gastrointestinal side effects are a common hurdle during dose escalation. Nausea affects about 17–22% of patients, diarrhea 13–16%, and vomiting 6–10%. While no dose adjustments are needed for patients with kidney or liver issues, healthcare providers should monitor for signs of dehydration-related acute kidney injury, especially when gastrointestinal symptoms are severe.
Efficacy Comparison: Weight Loss and Glycemic Control
Weight Loss Outcomes
Tirzepatide demonstrates more pronounced weight loss compared to semaglutide. In the SURPASS-2 trial, which included 1,879 patients with type 2 diabetes, a 15 mg dose of tirzepatide resulted in an average weight loss of 11.2 kg, significantly outpacing the 5.7 kg reduction observed with semaglutide 1 mg. This equates to a difference of –5.5 kg, a result that was statistically significant (P<0.001).
For individuals with obesity but without type 2 diabetes, a network meta-analysis revealed that tirzepatide 15 mg led to a 22.5% decrease in body weight, compared to 16.6–17.1% with semaglutide 2.4 mg. Additionally, tirzepatide showed a greater impact on waist circumference, reducing it by 5.32 cm more than semaglutide - a notable advantage for patients with central adiposity. These findings highlight tirzepatide's stronger effect on weight reduction, setting the stage for a deeper look into its glycemic control capabilities.
Glycemic Control Outcomes
Tirzepatide's dual receptor activity leads to better glucose regulation. In the SURPASS-2 trial, the 15 mg dose of tirzepatide lowered HbA1c levels by 2.30 percentage points, compared to a 1.86 percentage point reduction with semaglutide 1 mg. Even the lower 5 mg dose of tirzepatide surpassed semaglutide's effect, reducing HbA1c by 2.01 percentage points. Furthermore, 46% of patients on tirzepatide 15 mg achieved an HbA1c below 5.7%, compared to just 19% of those on semaglutide. Among patients starting with an HbA1c above 8.5%, tirzepatide 15 mg delivered a mean reduction of 3.22 percentage points.
Real-world data from 2025 reinforced these findings, showing that GLP-1–naïve patients initiating tirzepatide experienced a 1.3% HbA1c reduction, compared to a 0.9% reduction in those starting semaglutide.
"In patients with type 2 diabetes, tirzepatide was noninferior and superior to semaglutide with respect to the mean change in the glycated hemoglobin level from baseline to 40 weeks." - SURPASS-2 Investigators
Response Patterns and Durability
Both medications follow a similar trajectory, with improvements in weight and glycemic control accumulating during the titration phase and reaching a plateau around week 52. However, tirzepatide achieves a higher peak in weight loss before leveling off. On the other hand, semaglutide has shown stronger durability over the long term. For example, the SELECT trial, which tracked 17,604 adults with cardiovascular disease and obesity (but without type 2 diabetes), found that semaglutide 2.4 mg maintained a 10.2% mean weight reduction at 208 weeks, compared to just 1.5% in the placebo group.
Currently, tirzepatide lacks comparable long-term data beyond approximately 72 weeks, making semaglutide's extended efficacy particularly appealing for patients requiring sustained results. These differences in response patterns can guide treatment decisions based on individual patient needs.
Efficacy Metrics: Side-by-Side Table
| Metric | Tirzepatide 15 mg | Semaglutide (1 mg / 2.4 mg) | Difference |
|---|---|---|---|
| Weight loss (T2D patients) | 11.2 kg | 5.7 kg (1 mg) | –5.5 kg |
| Weight loss (obesity, no T2D) | ~22.5% | ~16.6–17.1% (2.4 mg) | Approximately –4.9% to –6.3% |
| HbA1c reduction | –2.30% | –1.86% (1 mg) | –0.44% |
| HbA1c <5.7% attainment | 46% | 19% (1 mg) | +27% |
| Waist circumference reduction | –12.30 cm | –6.98 cm (2.4 mg) | –5.32 cm |
| Long-term weight maintenance | Data pending beyond ~72 weeks | 10.2% at 208 weeks (2.4 mg) | - |
Data derived from the SURPASS-2 trial, network meta-analyses, and the SELECT trial.
Safety and Tolerability: Adverse Effects and Risks
Gastrointestinal Side Effects
Both tirzepatide and semaglutide are associated with gastrointestinal (GI) side effects like nausea, diarrhea, vomiting, constipation, and abdominal pain. These symptoms are usually mild to moderate, peaking during the titration phase before subsiding. A 2026 meta-analysis of 101 randomized controlled trials found that nausea occurred in 22.8% of patients, diarrhea in 13%, vomiting in 9.12%, and constipation in 7.39% of those treated with GLP-1 receptor agonists.
In the SURPASS-2 trial, tirzepatide showed higher rates of nausea and diarrhea compared to semaglutide, which had slightly more cases of vomiting and constipation. For tirzepatide, these effects were dose-dependent, with nausea increasing from 17.4% at 5 mg to 22.1% at 15 mg. Managing GI tolerance during titration is essential, and neither drug is suitable for individuals with severe gastroparesis. These tolerability issues lead into more serious risks associated with these therapies.
Serious Risks and Boxed Warnings
Both medications carry an FDA boxed warning for thyroid C-cell tumors based on rodent studies. They are contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Patients should report symptoms such as a neck mass, hoarseness, or swallowing difficulties immediately.
Acute pancreatitis is another serious risk, characterized by severe abdominal pain radiating to the back. Treatment should be discontinued if pancreatitis is suspected. Gallbladder issues, including gallstones and cholecystitis, have been reported and are often linked to rapid weight loss. Additionally, patients with pre-existing diabetic retinopathy need careful monitoring, as rapid glycemic control can temporarily worsen retinal complications. For instance, in one cardiovascular outcomes trial, 3% of semaglutide users experienced retinopathy complications compared to 1.8% in the placebo group.
Due to delayed gastric emptying, both drugs carry a risk of pulmonary aspiration during general anesthesia. Current guidelines suggest withholding weekly formulations one week before elective surgeries.
"Tirzepatide's overall safety data is similar to that of GLP-1 receptor agonists, except for hypoglycemia at doses higher than 10 mg." - StatPearls
Adherence and Discontinuation Rates
Adverse events not only affect patients' comfort but also influence their willingness to continue treatment. In the SURPASS-2 trial, discontinuation due to adverse events occurred in 6.0% of patients on tirzepatide 5 mg and 8.5% on the 10 mg and 15 mg doses, compared to 4.1% for semaglutide 1 mg. Serious adverse events were also more common with tirzepatide (5–7%) compared to semaglutide (3%). Gradual dose titration can help improve tolerance and reduce dropout rates.
Real-world data from 2025, involving over 20,000 patients, indicated that tirzepatide users might experience fewer GI and systemic adverse events compared to semaglutide users. This difference may stem from variations in patient selection or titration strategies.
Safety Metrics: Side-by-Side Table
The table below provides a direct comparison of safety metrics for tirzepatide and semaglutide.
| Safety Metric | Tirzepatide (5–15 mg) | Semaglutide (1 mg) |
|---|---|---|
| Nausea | 17.4% – 22.1% | 17.9% – 20.3% |
| Diarrhea | 13.2% – 16.4% | 8.8% – 11.5% |
| Vomiting | 5.7% – 9.8% | 8.1% – 9.2% |
| Constipation | 4.5% – 6.8% | 3.1% – 5.8% |
| Abdominal Pain | 3.0% – 5.1% | 5.1% – 5.7% |
| Pancreatitis | 0.4% | 0.6% |
| Discontinuation due to AEs | 6.0% – 8.5% | 4.1% |
| Serious Adverse Events | 5% – 7% | 3% |
| Boxed Warning | Thyroid C‑cell tumors | Thyroid C‑cell tumors |
Data derived from the SURPASS-2 trial, 2026 meta-analysis, and FDA prescribing information.
Prescribing Strategies: Practical Considerations
Matching Therapy to Patient Goals
When tailoring treatments to patient goals, it's essential to focus on outcomes that matter most to them. For example, weight loss is a common goal for non-diabetic patients. Studies show tirzepatide (10–15 mg) can lead to a 15–22% reduction in body weight, compared to 8–15% with semaglutide. Real-world data backs this up, with tirzepatide users losing an average of 10.2 kg over 12 months, compared to 6.1 kg with semaglutide.
For patients prioritizing glycemic control, both medications are effective. However, tirzepatide's dual GIP/GLP-1 action may provide added benefits, especially for those with significant obesity, cardiometabolic risks, or challenges achieving optimal glucose levels with GLP-1 monotherapy.
If a patient achieves less than 5% weight loss after six months on the highest tolerated dose, it’s time to reassess the treatment plan.
"If less than 5% of the initial weight has been lost after 6 months on the highest tolerated dose, decide whether to continue treatment, taking into account the benefits and risks of treatment for the person." - National Institute for Health and Care Excellence (NICE)
Switching Between Agents
When a patient doesn’t tolerate their current medication or fails to meet their goals, switching therapies can be a practical solution. However, it’s important to approach this transition carefully. Start with the lowest dose - 0.25 mg weekly for semaglutide or 2.5 mg weekly for tirzepatide - and follow the standard 4-week titration schedule.
The timing of the switch depends on the patient’s circumstances. For those with significant side effects, a 1–2 week washout period is recommended. On the other hand, stable patients with minimal gastrointestinal issues can begin the new medication on their next scheduled dosing day. Patients should be informed that a temporary weight plateau or slight weight regain is normal during the re-titration phase.
"The safest approach is to restart semaglutide at its lowest available dose (i.e. 0.25mg weekly), then titrate gradually per standard schedule, regardless of the previous tirzepatide dose." - Sehar Shahid, Clinical Trainer, Eli Lilly
For patients using oral contraceptives, switching to or increasing the dose of tirzepatide requires extra caution. They should use a backup barrier method for three weeks after each dose adjustment, as delayed gastric emptying can affect oral contraceptive absorption.
These protocols highlight the need for careful monitoring during any treatment transition.
Monitoring and Documentation
Once adjustments are made, ongoing monitoring is critical to ensure the treatment remains effective and safe. Regular check-ins help confirm that the benefits observed in clinical trials are being achieved. Below is a summary of key parameters to monitor and how frequently they should be checked:
| Parameter | Frequency | Why It Matters |
|---|---|---|
| Weight, BMI, Waist Circumference | Baseline; monthly during titration, then every 3–6 months | Tracks progress in weight management |
| HbA1c | Every 3 months | Assesses glycemic control in diabetic patients |
| Fasting Plasma Glucose | Daily (for insulin users) | Identifies risks of hypoglycemia |
| Renal Function (eGFR/Creatinine) | If severe gastrointestinal symptoms occur | Prevents dehydration-related kidney issues |
| Resting Heart Rate | Baseline, 12 weeks, then every 6 months | Tirzepatide may increase heart rate by 2–10 bpm |
| INR (if on Warfarin) | Weeks 1, 2, and 4 after titration | Monitors for fluctuations due to delayed absorption |
| TSH (if on Levothyroxine) | 3 months post-titration | Ensures thyroid hormone levels remain stable |
Incorporating Quality of Life (QOL) tools, such as the Diabetes Quality of Life (DQoL) measure, during routine visits adds another layer of insight. These tools can help track patient-reported outcomes like mood, energy, and appetite. Always document titration decisions, tolerability evaluations, and the reasons for switching medications to maintain continuity of care and meet regulatory standards.
The Weight Loss Showdown: Semaglutide vs. Tirzepatide Head-to-Head Study: IM Grand Rounds
Regulatory and Access Considerations
This section delves into the regulatory guidelines, pricing structures, and documentation practices that influence prescribing decisions.
FDA Approvals and Off-Label Use
The FDA-approved uses for each medication play a significant role in guiding prescribing practices. Semaglutide is approved for managing type 2 diabetes (Ozempic, 2017; Rybelsus, 2019), chronic weight management (Wegovy, 2021), and reducing cardiovascular risks. Similarly, Tirzepatide is approved for type 2 diabetes (Mounjaro, 2022), chronic weight management (Zepbound, 2023), and treating obstructive sleep apnea in adults with obesity (Zepbound, 2024).
In some cases, Mounjaro is prescribed off-label for obesity when Zepbound isn't available. Before starting either medication, ensure contraindications are screened and documented as previously outlined.
Cost and Insurance Coverage
The cost of these medications varies depending on the brand, formulation, and patient access. As of April 2026, the monthly U.S. list prices for injectable branded options range between $935 and $1,349. Tirzepatide (Zepbound) is priced at approximately $1,060 per month, making it about 21% less expensive than Wegovy's $1,349 monthly cost. This makes Zepbound a more affordable choice for patients paying out of pocket.
Eli Lilly offers a LillyDirect program, which provides Zepbound at $299–$550 per month through December 2026, making it the most affordable branded injectable option currently available. For patients with commercial insurance, copays typically range from $25 to $50 per month if the medication is on the formulary. About 65% of commercial insurance plans cover Wegovy, while around 60% cover Zepbound.
A major change occurred in 2026 when Medicare began covering both Wegovy and Zepbound under Part D for weight management, reversing its previous exclusion. Additionally, a Medicare Bridge program, launching on July 1, 2026, will cap out-of-pocket costs at $50 per month for eligible enrollees. Patients relying on Medicare should consider this timeline if cost has been a hurdle.
These pricing and coverage factors significantly influence patient access and adherence to treatment.
| Medication | List Price (Monthly) | Cash/Direct Price |
|---|---|---|
| Wegovy (Semaglutide, injectable) | $1,349 | $1,349 |
| Ozempic (Semaglutide, injectable) | $935 | $935 |
| Oral Wegovy (Semaglutide, pill) | $199–$299 | $199–$299 |
| Zepbound (Tirzepatide, injectable) | $1,060 | $299–$550 (LillyDirect) |
| Mounjaro (Tirzepatide, injectable) | $1,060 | $1,060 |
Documentation for Compliance
Accurate documentation not only ensures regulatory compliance but also supports better patient outcomes.
For patients prescribed these medications, record a BMI ≥30 kg/m² or ≥27 kg/m² with at least one weight-related comorbidity (such as hypertension or type 2 diabetes). Include evidence of lifestyle interventions and confirm the absence of contraindications like MTC or MEN-2, as per earlier guidelines. Additionally, document baseline and follow-up HbA1c levels for both clinical management and insurance purposes.
Two often-overlooked areas of documentation include ocular monitoring and psychological assessments. Clinical trials for Semaglutide (Ozempic) reported a 3.0% incidence of diabetic retinopathy complications compared to 1.8% for placebo, so patients with a history of retinopathy should undergo baseline eye exams. For those using Wegovy for weight loss, monitor for any new or worsening signs of depression or suicidal thoughts, and document these evaluations at each visit. If a patient is preparing for surgery, ensure documentation reflects that they’ve been advised to inform their anesthesia team about GLP-1 use, as it can delay gastric emptying.
Conclusion: Key Takeaways for Prescribers
This summary highlights the critical points from the clinical review, offering a guide to making informed treatment decisions. Semaglutide and Tirzepatide each bring unique advantages that cater to different patient needs. The choice between them depends on the primary treatment goal - whether it's focused on weight loss, organ protection, preferred administration method, or addressing a specific condition like obstructive sleep apnea.
When to Use Semaglutide vs. Tirzepatide
Consider Semaglutide when cardiovascular or kidney protection is a top priority. The SELECT trial demonstrated a 20% reduction in MACE for patients with obesity and cardiovascular disease, even without diabetes. Additionally, Semaglutide gained FDA approval in January 2025 for slowing the progression of chronic kidney disease in adults with type 2 diabetes, showing a 24% reduction in CKD advancement. For patients who prefer oral medication or have a fear of needles, Semaglutide is the only option in this class available as a daily oral tablet (Rybelsus).
Opt for Tirzepatide when maximum weight loss or aggressive glycemic control is the goal. A 2026 meta-analysis found that Tirzepatide 15 mg achieves a 6.10% greater mean weight loss compared to Semaglutide 2.4 mg, along with a 5.32 cm greater reduction in waist circumference. It also provides superior HbA1c reduction by −0.44 percentage points at the 15 mg dose. For patients with moderate-to-severe obstructive sleep apnea, Tirzepatide (Zepbound) stands out as the only FDA-approved treatment in this class for that condition, with approval granted in December 2024.
However, Tirzepatide carries a higher risk of clinically significant hypoglycemia (glucose <54 mg/dL), affecting 1.7% of patients on the 15 mg dose compared to 0.4% on Semaglutide 1 mg. This necessitates careful insulin adjustments and closer monitoring during initiation.
Final Comparison Table
| Factor | Semaglutide (Wegovy/Ozempic) | Tirzepatide (Zepbound/Mounjaro) |
|---|---|---|
| Mechanism | Selective GLP-1 RA | Dual GIP/GLP-1 RA |
| Avg. Weight Loss | ~15% | ~20–22% |
| HbA1c Reduction (vs. each other) | Baseline reference | −0.44 pp greater at 15 mg |
| CV Benefit | 20% MACE reduction (SELECT) | Pending (SURPASS-CVOT) |
| Kidney Protection | FDA-approved for CKD (Jan 2025) | Earlier-stage data only |
| Sleep Apnea (OSA) | Not FDA-approved | FDA-approved (Dec 2024) |
| Administration | Weekly injection or daily oral | Weekly injection only |
| Hypoglycemia Risk | 0.4% at 1 mg | 1.7% at 15 mg |
| Oral Contraceptive Interaction | Not specifically flagged | Reduced efficacy during initiation/escalation |
These comparisons provide the clarity prescribers need to tailor treatments to individual patient profiles and clinical objectives. Each medication offers distinct strengths that can be matched to specific therapeutic goals.
FAQs
Which patients should get semaglutide instead of tirzepatide?
Patients who have experienced severe gastrointestinal (GI) side effects with other medications might find semaglutide easier on their system, as it tends to cause fewer GI issues. For those managing costs, semaglutide is often a more budget-friendly choice, particularly for individuals paying out of pocket. Additionally, oral semaglutide provides a great option for people who are uncomfortable with needles or don’t have insurance coverage for injectable medications, offering a convenient, non-injectable alternative.
How do I switch a patient between semaglutide and tirzepatide safely?
Switching from semaglutide to tirzepatide (or vice versa) requires careful management and should always be done under a physician's guidance. Here’s how the process typically works:
- Allow for a 3–7 day washout period between stopping one medication and starting the other. This helps to minimize any overlapping effects.
- Begin the new medication at its lowest possible dose to reduce the risk of side effects.
- Gradually increase the dosage over several weeks, following the prescribed titration schedule.
- Keep a close eye on potential side effects, particularly gastrointestinal issues, and make adjustments if necessary.
Regular follow-ups with your healthcare provider are crucial during this transition. These check-ins not only help monitor your progress but also ensure that you're educated about the process, making the treatment safer and more effective.
What monitoring should I do during titration to reduce risk?
When adjusting doses of Semaglutide or Tirzepatide, it's essential to keep an eye on key health indicators:
- Blood glucose and HbA1c levels: These help track how well the treatment is working.
- Gastrointestinal symptoms: Be mindful of issues like nausea, vomiting, or diarrhea. Adjust the dosage if these symptoms become problematic.
- Pancreatitis warning signs: Severe abdominal pain could indicate pancreatitis and requires immediate attention.
- Renal function: Patients at risk for kidney problems should be closely monitored.
- Thyroid tumor symptoms (specific to Tirzepatide): Look out for signs like a neck mass or unusual swelling.
By staying vigilant, you can help minimize risks and improve the effectiveness of these treatments.