
New treatments for obesity are targeting the gut-brain axis, offering promising results for weight loss. These therapies leverage peptides like GLP-1, GIP, and amylin to regulate hunger, energy use, and metabolism. Traditional methods often fall short, but next-generation drugs like tirzepatide, retatrutide, and CagriSema are showing improved outcomes by activating multiple hormonal pathways. Here's a quick overview:
- Tirzepatide (Zepbound): FDA-approved dual GLP-1/GIP agonist, delivering up to 22.4% weight loss over 72 weeks.
- Retatrutide: Triple GLP-1/GIP/glucagon agonist with up to 28.3% weight loss in trials, pending FDA approval.
- CagriSema: Combines GLP-1 and amylin for 22.7% weight loss, awaiting FDA decision in 2026.
Non-incretin therapies like amylin and PYY analogs are also emerging, addressing unique pathways to improve satiety and preserve lean body mass. While these treatments are effective, they come with challenges like gastrointestinal side effects and the need for peptide dosing protocols for gradual adjustments. The future of obesity care lies in combining these advanced approaches to achieve sustainable results.
The New Science of Weight Loss: From Brain Biology to GLP-1s
sbb-itb-7164bd9
Next-Generation Incretin and Multi-Agonist Peptides
The evolution from single-receptor GLP-1 agonists to multi-target peptides represents a logical progression in peptide therapies. By engaging multiple hormonal pathways simultaneously, these agents deliver stronger and longer-lasting effects. Let’s take a closer look at three leading contenders in this space.
Tirzepatide: Dual GIP/GLP-1 Receptor Agonist
Tirzepatide, often referred to as a "twincretin", is a 39-amino acid peptide that activates both GLP-1 and GIP receptors. It has a fivefold higher binding affinity for GIP receptors compared to GLP-1, which contributes to better gastrointestinal tolerability and improved insulin sensitivity in white adipose tissue.
In the SURMOUNT-1 trial, participants without diabetes experienced weight loss ranging from 16.5% to 22.4% over 72 weeks, depending on the dose (5 mg to 15 mg). The SURMOUNT-5 trial further demonstrated tirzepatide’s superiority over semaglutide 2.4 mg in reducing both body weight and waist circumference at week 72, with fewer participants discontinuing treatment due to gastrointestinal issues (2.7% vs. 5.6%). As of June 2026, tirzepatide is FDA-approved for chronic weight management under the name Zepbound and for type 2 diabetes as Mounjaro.
Retatrutide: Triple GLP-1/GIP/Glucagon Agonist
Retatrutide takes the incretin approach further by adding glucagon receptor activation to the mix. While GLP-1 and GIP regulate appetite and insulin, glucagon promotes energy expenditure and liver fat reduction.
"The triple agonist is essentially a thermogenic-plus-anorexigenic combination in one molecule." - J. Amirzada, Editor-in-Chief, Wellness Radar
In May 2026, Eli Lilly shared results from the TRIUMPH-1 Phase 3 trial, led by Dr. Ania Jastreboff of Yale School of Medicine. Among 2,339 participants, those on the 12 mg dose achieved an average weight loss of 28.3% (70.3 lbs) at 80 weeks, with 45.3% losing at least 30% of their body weight. For participants with a baseline BMI of 35 or higher who continued to 104 weeks, the average weight loss reached 30.3% (85.0 lbs). Additionally, Phase 2 data revealed an 84.2% reduction in liver fat, a promising sign for individuals with metabolic-associated steatotic liver disease. Retatrutide remains investigational as of June 2026, pending FDA approval.
CagriSema: Amylin Analog and GLP-1 Agonist in Fixed-Dose Combination
CagriSema pairs cagrilintide (an amylin analog) with semaglutide to target different central nervous system pathways. Amylin enhances feelings of fullness and reduces glucagon, while GLP-1 slows gastric emptying and curbs appetite. Together, these mechanisms achieve outcomes that neither agent could produce alone.
In the REDEFINE 1 trial, which included 3,417 adults without diabetes, CagriSema resulted in a 22.7% weight loss at 68 weeks, outperforming semaglutide alone (16.1%) and cagrilintide alone (11.8%). Remarkably, 54% of participants reduced their BMI below 30 kg/m², moving out of the obesity category by week 68. In December 2025, Novo Nordisk submitted a New Drug Application (NDA) to the FDA, with a decision expected in 2026.
"The FDA submission of CagriSema marks an important milestone and signals a new era in weight management, reinforcing Novo Nordisk's long-standing commitment to serving people living with obesity through innovation and science." - Mike Doustdar, President and CEO, Novo Nordisk
Here’s a quick comparison of these peptides:
| Peptide | Receptors Targeted | Key Trial | Weight Loss | FDA Status (June 2026) |
|---|---|---|---|---|
| Tirzepatide | GLP-1 + GIP | SURMOUNT-1 | Up to 22.4% (72 weeks) | Approved (Zepbound) |
| Retatrutide | GLP-1 + GIP + Glucagon | TRIUMPH-1 | 28.3% (80 weeks) | Investigational (Phase 3) |
| CagriSema | GLP-1 + Amylin | REDEFINE 1 | 22.7% (68 weeks) | NDA Submitted Dec 2025 |
Amylin Analogs and PYY-Based Peptides: Non-Incretin Gut-Brain Targets
As multi-agonist therapies continue to evolve in obesity treatment, non-incretin pathways are emerging as powerful allies. While incretin-based therapies like GLP-1, GIP, and glucagon receptor agonists dominate the field, amylin and peptide YY (PYY) are gaining attention for their distinct roles in appetite regulation. These gut-brain signals operate through unique mechanisms, opening up new possibilities for managing obesity.
Amylin Analogs: A Dual Approach
Amylin, a 37-amino acid hormone, is co-released with insulin from pancreatic beta cells. It plays a key role in regulating appetite by increasing satiety, slowing gastric emptying, and suppressing post-meal glucagon secretion. These effects are primarily mediated through receptors in the area postrema of the hindbrain, leading to fat loss while preserving lean body mass.
The challenge with native amylin lies in its short half-life - less than 20 minutes - which has driven the development of long-acting analogs. For instance, Cagrilintide has shown significant promise in reducing fat mass while maintaining lean tissue. Building on this, Novo Nordisk is advancing Amycretin, a dual-acting molecule targeting both GLP-1 and amylin receptors. Early trials have reported a notable 24% weight reduction over 36 weeks in Phase 1b/2a studies.
"Amylin-based medicines might eventually be used to address different diseases of the metabolic spectrum, namely obesity and its complications." - Diabetes Therapy
While amylin analogs focus on hindbrain-driven appetite control, PYY-based therapies take a different route, leveraging hypothalamic pathways to enhance satiety.
PYY-Targeting Peptides: Amplifying Fullness Signals
Peptide YY (PYY) is a 36-amino acid hormone released by L-cells in the distal gut after eating, especially in response to protein and calorie intake. PYY(3-36) binds to Y2 receptors in the arcuate nucleus of the hypothalamus, where it suppresses hunger-inducing NPY/AgRP neurons and activates satiety-promoting POMC neurons. Additionally, PYY slows gastric motility through the "ileal brake", prolonging the feeling of fullness.
In individuals with obesity, fasting PYY levels are often lower, and the post-meal response is diminished. This "PYY deficiency" means that people with obesity require nearly double the caloric intake to achieve similar circulating levels of PYY as lean individuals. Addressing this gap, researchers are developing stable, long-acting PYY analogs. For example, PYY1875 uses fatty acid modification to enable weekly dosing. Preclinical studies combining PYY with GLP-1 have shown enhanced weight loss and better blood sugar control, without the rapid muscle loss that can accompany extreme calorie restriction.
| Feature | Amylin Analogs | PYY-Based Therapies |
|---|---|---|
| Primary Source | Pancreatic beta cells | Distal gut L-cells |
| Brain Target | Hindbrain (Area Postrema) | Hypothalamus (Arcuate Nucleus) |
| Key Satiety Mechanism | Slows gastric emptying; reduces glucagon | Inhibits NPY/AgRP neurons; activates POMC neurons |
| Body Composition Benefit | Preserves lean mass | May maintain muscle mass |
| Key Clinical Agents | Cagrilintide, Amycretin | PYY1875 (investigational) |
Ghrelin-Axis Modulators and Other Novel Gut-Brain Targets
Modulating the Ghrelin System for Appetite Control
Ghrelin plays a key role in hunger regulation by activating neuropeptide Y (NPY) and agouti-related peptide (AgRP) neurons in the hypothalamic arcuate nucleus. This disrupts satiety signals mediated by the MC4R pathway, essentially serving as the brain's "time to eat" signal.
To counteract this, researchers have tested several approaches. For instance, GOAT inhibitors like BI 1356225 can cut acyl-ghrelin levels by more than 80%. Similarly, endogenous inverse agonists such as LEAP2 work by counteracting ghrelin's effects at the GHSR1a receptor. However, challenges remain. None of these strategies have reached the U.S. market as of mid-2026 due to inconsistent results in efficacy and safety testing. One notable example is livoletide, a des-acyl ghrelin analog, which was discontinued after failing to meet its efficacy goals in Phase 3 trials.
While ghrelin modulation holds promise, researchers are also exploring other gut-brain pathways to tackle obesity.
Nesfatin-1, OXM Analogs, and Other Emerging Targets
Beyond ghrelin, other peptides like nesfatin-1 and oxyntomodulin (OXM) present alternative mechanisms for managing energy balance. Nesfatin-1 has shown encouraging results in preclinical studies for appetite control, though its therapeutic potential is still in the early stages of research. On the other hand, OXM is more advanced in development. Acting as a natural dual agonist for GLP-1 and glucagon receptors (GCGR), it reduces appetite through GLP-1 receptor activation while boosting energy expenditure via GCGR stimulation.
Another exciting candidate is BRP, a 12-amino acid peptide discovered through computational screening. In preclinical models, BRP not only reduced food intake but also reversed obesity, all without triggering nausea. A 2025 study led by Katrin J. Svensson at Stanford University highlighted its effectiveness in both mice and minipigs. Interestingly, BRP activates central FOS signaling in the hypothalamus without relying on the GLP-1 receptor, leptin, or MC4R.
"BRP administration triggers central FOS activation and acts independently of leptin, GLP-1 receptor and melanocortin 4 receptor." - Nature Portfolio
This independence from the GLP-1 pathway makes BRP a potential option for patients who don't respond well to GLP-1-based therapies, fitting specific patient selection criteria. It could also benefit those who hit a plateau with such treatments. Researchers are increasingly focusing on "mechanism stacking" - combining different pathways to enhance weight loss while minimizing side effects.
Clinical Integration and the U.S. Regulatory Landscape
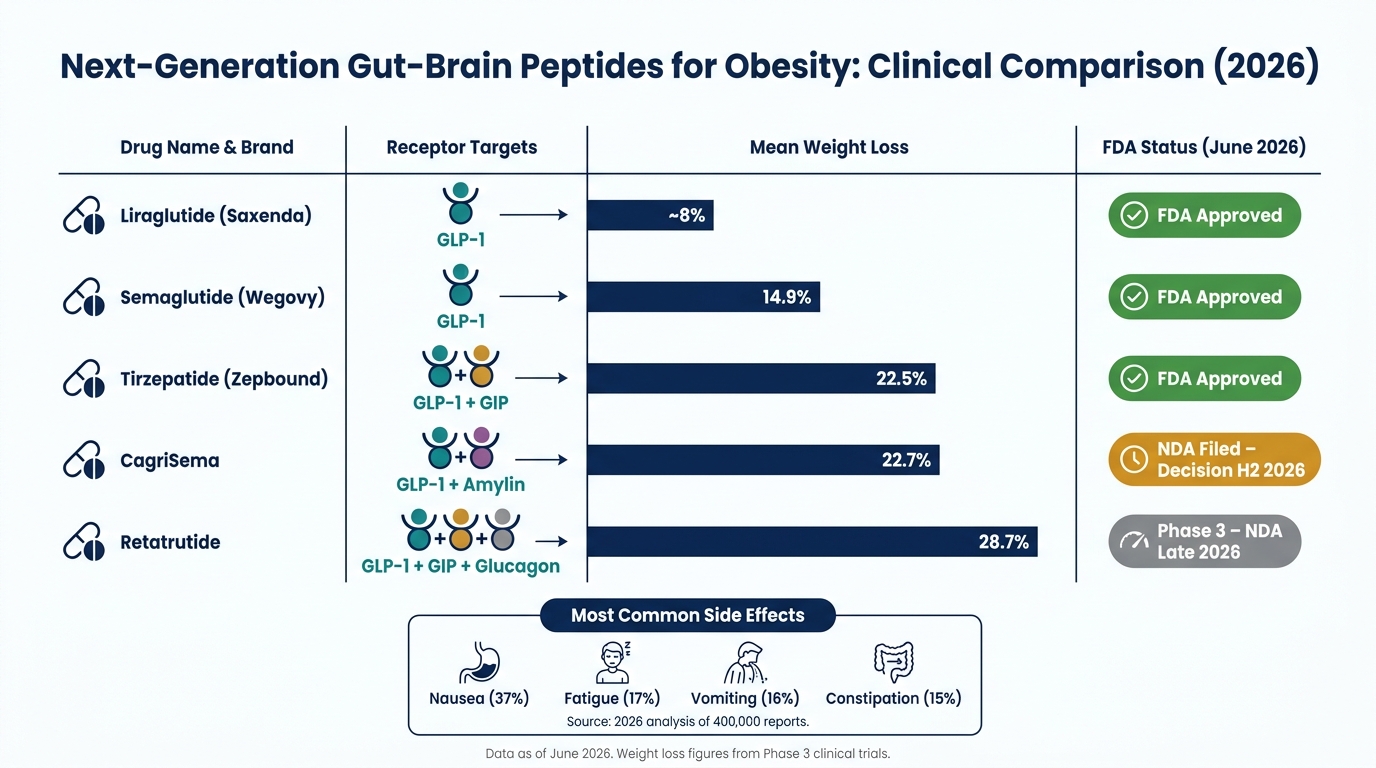
Next-Gen Obesity Peptides: Weight Loss Results & FDA Status (2026)
FDA Approvals and Investigational Therapies: Current Status
By June 2026, five peptide-based medications have received FDA approval for managing chronic weight conditions: Wegovy (semaglutide injection), Zepbound (tirzepatide), Saxenda (liraglutide), a high-dose oral semaglutide tablet approved in late 2025, and IMCIVREE (setmelanotide). Notably, in March 2026, IMCIVREE became the first therapy approved specifically for acquired hypothalamic obesity in children as young as four years old.
The development pipeline for weight-management therapies is also bustling. CagriSema had its New Drug Application (NDA) filed in December 2025, with the FDA expected to make a decision in the latter half of 2026. Meanwhile, Retatrutide, which demonstrated an impressive 28.7% average weight reduction over 68 weeks in the TRIUMPH-4 Phase 3 trial, is gearing up for an NDA submission by late 2026. The table below outlines the status of key therapies as of June 2026:
| Compound | Receptor Targets | Mean Weight Loss | Status (June 2026) |
|---|---|---|---|
| Liraglutide | GLP-1 | ~8% | FDA Approved |
| Semaglutide | GLP-1 | 14.9% | FDA Approved |
| Tirzepatide | GLP-1 / GIP | 22.5% | FDA Approved |
| CagriSema | GLP-1 / Amylin | 22.7% | NDA Filed (Decision H2 2026) |
| Retatrutide | GLP-1 / GIP / Glucagon | 28.7% | Phase 3 (NDA Late 2026) |
The resolution of semaglutide and tirzepatide shortages in late 2024 and early 2025 effectively ended the legal grounds for routine 503A compounding of these drugs. Under the FD&C Act, no clear legal framework currently exists for patient-specific compounding of these molecules. While regulatory milestones highlight their availability, attention to safety profiles remains a top priority.
Safety Considerations for Gut-Brain Peptides
Gastrointestinal side effects dominate the safety profile of these therapies. A 2026 analysis of 400,000 reports identified nausea (37%), fatigue (17%), vomiting (16%), and constipation (15%) as the most commonly reported issues. To minimize these effects, gradual dose titration remains the standard practice across this drug class.
GLP-1 receptor agonists and dual agonists carry a boxed warning for medullary thyroid carcinoma (MTC) and multiple endocrine neoplasia syndrome type 2 (MEN2). Screening for personal or family history of these conditions is essential before initiating treatment. Additionally, clinicians should monitor for acute kidney injury, especially in patients experiencing significant gastrointestinal fluid loss, and remain vigilant for signs of acute pancreatitis.
Emerging therapies bring new challenges. For example, Retatrutide was associated with dysesthesia (abnormal skin sensations) in 20.9% of participants at the 12 mg dose during Phase 3 trials. This side effect is tied to its glucagon-receptor activity, which is not observed with GLP-1–only therapies. As research progresses into triple and multi-agonist therapies, monitoring protocols will need to address these evolving safety concerns.
Another key consideration is the effect of these drugs on oral contraceptive absorption. Tirzepatide significantly delays gastric emptying, which can reduce the efficacy of oral hormonal contraceptives. To mitigate this risk, patients should switch to non-oral or barrier contraceptive methods for four weeks after starting treatment and after each dose escalation.
"Weight regain after discontinuation is the rule, not the exception. Plan the maintenance question before starting the protocol." - Klarovel Medical Advisory Board
Clinical Resources to Support Safe and Informed Prescribing
With regulatory changes and expanding safety data, access to reliable clinical resources is critical for healthcare providers navigating this complex field. For those prescribing these therapies, combining up-to-date regulatory knowledge with effective clinical tools is key to ensuring the best outcomes for patients.
PeptidePrescriber offers a comprehensive platform tailored to licensed healthcare professionals. It includes detailed peptide monographs, dosing protocols, regulatory references, and practical tools like reconstitution calculators and injection site guides - all designed to streamline clinical practice.
For clinicians new to peptide therapies, the platform also provides guidance on compliance, sourcing, and building a legally sound practice. Its prescriber network fosters collaboration and knowledge-sharing, making it a valuable resource for those entering this rapidly evolving field.
Conclusion: What Gut-Brain Peptides Mean for the Future of Obesity Care
The move from single-target treatments to therapies that engage multiple receptors is reshaping how obesity is managed. Peptides like tirzepatide and retatrutide go beyond simply curbing appetite - they activate several regulatory pathways in a way that single-pathway drugs just can’t match. This broader approach has led to unprecedented weight-loss outcomes, with triple agonists now achieving reductions of over 28%. These results were once only possible through bariatric surgery.
New targets beyond incretins are also broadening the scope of treatment, offering effective weight-loss options with different side-effect profiles.
However, clinical success depends on more than just efficacy. Navigating evolving regulations and addressing individual patient needs require reliable, evidence-based tools. Platforms like PeptidePrescriber equip licensed prescribers with essential clinical guides, including dosing guidelines, regulatory insights, and safety protocols, making it easier to handle the complexities discussed in this review.
The direction is clear: obesity treatment is embracing rational polypharmacology, with multi-agonist therapies leading the way by targeting multiple complementary pathways in a single drug. For healthcare providers, staying informed isn’t just helpful - it’s essential for delivering safe and effective care.
FAQs
How do multi-agonist peptides work differently than GLP-1 alone?
Multi-agonist peptides take a different route than GLP-1 mono-agonists by targeting multiple hormonal pathways instead of focusing on just one. While GLP-1 mono-agonists primarily regulate appetite and insulin through a single signaling mechanism, multi-agonists go further. They activate additional receptors like GIP and glucagon, which help boost fat oxidation, promote lipolysis, and increase energy expenditure.
This combination of actions mirrors the body’s natural processes more effectively, leading to stronger and more sustained outcomes compared to GLP-1 monotherapy.
Who should avoid these obesity peptides due to safety warnings?
Safety warnings depend heavily on the type of peptide in question. Peptides that haven't been approved often come with risks tied to their unverified origins and the absence of thorough safety testing. On the other hand, FDA-approved GLP-1 receptor agonists can cause side effects such as nausea, constipation, and even muscle loss. Precision therapies like setmelanotide are specifically designed for individuals with certain genetic mutations and are not intended to treat general cases of obesity.
What happens if you stop taking these medications?
When people stop using weight-loss peptides like GLP-1 receptor agonists, weight regain is common. These medications work by curbing appetite and influencing metabolism, so without them, the body often reverts to its previous state. Studies reveal that most individuals regain the weight they lost within 1.5 to 2 years after stopping the treatment. That said, some manage to keep the weight off by sticking to ongoing lifestyle changes, such as maintaining a regular exercise routine. It's worth noting that obesity is now widely regarded as a chronic condition that requires ongoing management rather than a short-term fix.