
Peptides are becoming a bigger part of medicine, but understanding their research can be tricky. Many peptides are marketed based on limited animal studies, and safety concerns are growing, with cases of adverse events and even deaths tied to unregulated use. This guide helps clinicians critically evaluate peptide research, prioritize patient safety, and stay compliant with U.S. regulations.
Key Takeaways:
- Evidence Matters: Human trials are more reliable than animal studies. Peptides like Semaglutide have strong evidence, while others like BPC-157 lack robust human data.
- Regulatory Classifications: Know whether a peptide is FDA-approved, compounded, or unregulated. Avoid using "Research Use Only" peptides in patients.
- Safety First: Always verify dosing, monitor for side effects, and source peptides from licensed 503A/503B pharmacies.
- Critical Reading: Understand study designs, populations, and endpoints. Focus on patient-centered outcomes over surrogate markers.
Peptide therapy can be useful, but only when backed by solid evidence and thoughtful clinical judgment.
Are Peptides a Miracle Drug or a Risky Gamble (Doctor Explains)
For a deeper dive into the science, see our clinical overview of peptide therapy.
sbb-itb-7164bd9
What to Look for When Reviewing Peptide Research
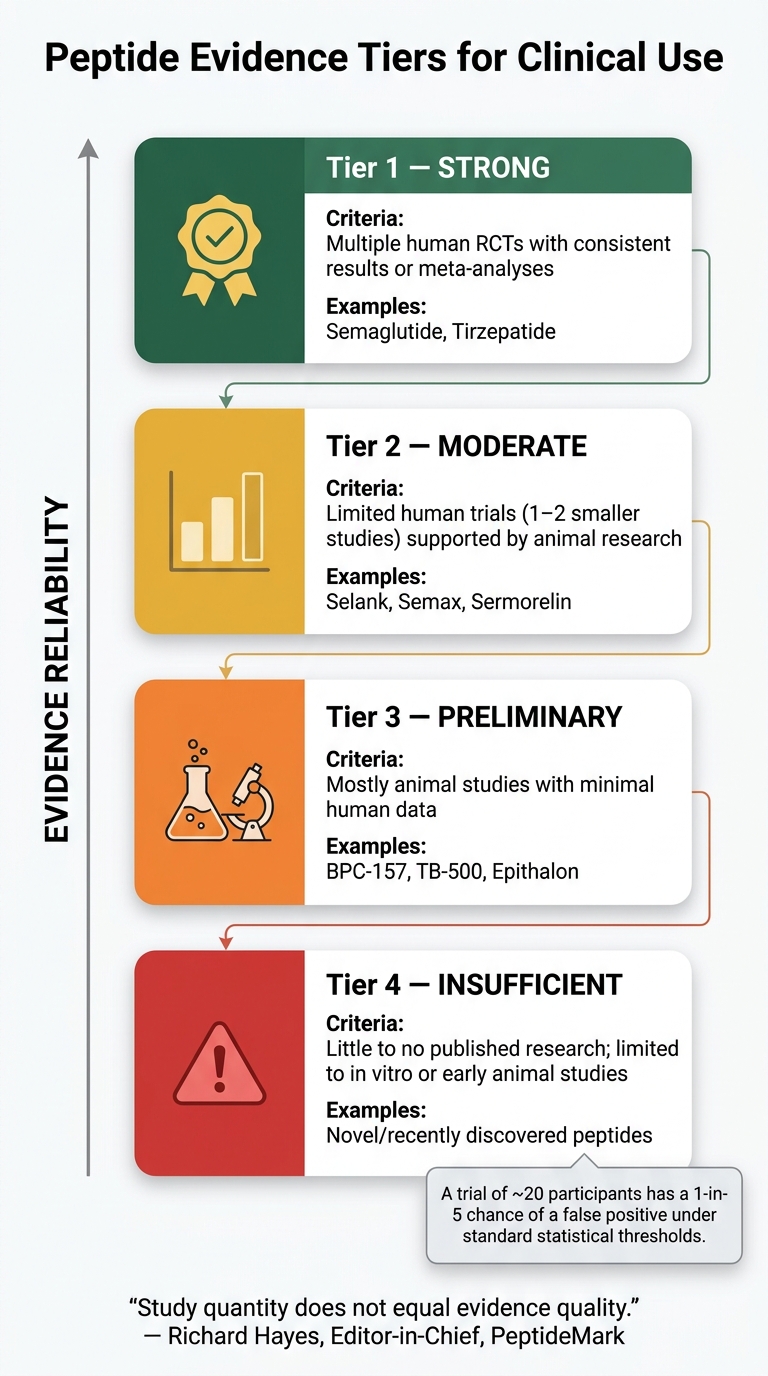
Peptide Evidence Tiers: From Strong to Insufficient
Understanding the Evidence Hierarchy
Peptide research comes with varying levels of reliability, and it's essential to understand the evidence hierarchy. At the top, you’ll find systematic reviews and meta-analyses of randomized controlled trials (RCTs) - the gold standard for reliable data. As you move down the hierarchy, the reliability decreases, passing through cohort studies, case series, animal models, and, finally, cell cultures. For evidence to be considered strong, it typically requires multiple human RCTs with consistent findings or a single, well-designed RCT with more than 500 participants.
Here’s a breakdown of peptides by evidence tier:
| Evidence Tier | Criteria | Examples |
|---|---|---|
| Strong | Multiple human RCTs with consistent results or meta-analyses | Semaglutide, Tirzepatide |
| Moderate | Limited human trials (1–2 smaller studies) supported by animal research | Selank, Semax, Sermorelin |
| Preliminary | Mostly animal studies with minimal human data | BPC-157, TB-500, Epithalon |
| Insufficient | Little to no published research; limited to in vitro or early animal studies | Novel/recently discovered peptides |
Source:
It’s worth noting that a small trial involving around 20 participants has about a 1-in-5 chance of producing a false positive under standard statistical thresholds. This highlights the importance of interpreting limited data cautiously.
"Study quantity does not equal evidence quality. Until meaningful human clinical trial data is available, the evidence remains preliminary regardless of how many preclinical studies exist." - Richard Hayes, Editor-in-Chief, PeptideMark
Understanding these evidence tiers is crucial when evaluating peptides, especially when considering their regulatory status.
FDA-Approved vs. Experimental Peptides
Knowing a peptide's regulatory classification is just as important as understanding the science behind it. Peptides fall into four main categories: FDA-approved drugs, lawfully compounded peptides (503A/503B pharmacies), "Research Use Only" (RUO) compounds, and peptides within the wellness/telehealth "gray zone".
- FDA-approved peptides: These have undergone the rigorous New Drug Application (NDA) process, are manufactured under cGMP standards, and include specific labeled uses.
- Compounded peptides: These come from 503A or 503B pharmacies. While not FDA-approved, they operate within defined regulatory frameworks. Facilities under 503B regulations face stricter cGMP requirements and FDA inspections compared to 503A pharmacies.
- Research Use Only (RUO) products: Despite the name, RUO is a vendor disclaimer, not an official regulatory category. These peptides are intended for in vitro research only and may contain hazardous solvents like trifluoroacetic acid (TFA). Using RUO products for patient administration carries significant liability risks.
"RUO products are not intended for patient administration... Approved levels of hazardous solvents in synthesizing and purifying peptides are different for RUO and medically graded peptides." - Benjamin González, MD, Integrative and Functional Medicine Physician
Understanding these classifications ensures safer prescribing practices and compliance with U.S. regulations.
Study Design and Data Quality
When assessing peptide studies, take a close look at the methods section. Key details to evaluate include the study type, sample size, control groups, and whether the study was pre-registered. Pre-registration is critical because it prevents outcome reporting bias - the selective publication of favorable results. Additionally, check for both p-values and confidence intervals, as they help gauge the magnitude and precision of the findings. Be cautious with industry-funded trials or studies replicated by a single source, as these can sometimes exaggerate effect sizes.
How to Read and Appraise a Peptide Study
Start With a Clear Clinical Question
Before diving into a peptide study, it’s essential to have a well-defined clinical question. This helps you stay focused and avoid being overly influenced by the study’s conclusions before examining its details. Consider questions like: Does this peptide specifically address my patient’s condition? Was it tested in a population similar to theirs? What dose and route were used? Without this framework, there’s a risk of misapplying results to situations they weren’t designed to address.
When reading the study, start with the methods section rather than the abstract. Abstracts often highlight positive outcomes while downplaying limitations. The methods section, however, offers a more accurate picture of the study’s quality and potential weaknesses.
Next, evaluate whether the study design is relevant to your clinical context.
Review Study Populations and Dosing Regimens
Once you’ve clarified your clinical question, assess whether the study’s population and dosing regimens align with your practice. Research conducted on young, healthy adults might not apply to older patients with multiple health conditions or those on several medications. Pay close attention to the inclusion and exclusion criteria - if the study excluded individuals with conditions common in your patient population, its findings may have limited relevance.
Dosing is another critical factor. Peptides often behave differently depending on the delivery method, so results from one formulation or route can’t be directly applied to another. For example, a study using one delivery method doesn’t automatically justify using a different one. If the study is preclinical, check whether the researchers used allometric scaling to estimate human-equivalent doses. Simple weight-based calculations from animal data are not accurate and can result in dosing errors.
Also, watch for any gaps between the study’s indication and your intended use. For instance, while much of the BPC-157 research focuses on gut injury models, that doesn’t mean the findings apply to tendon or ligament injuries in humans.
Assess Outcomes and Safety Signals
The final step is to weigh the benefits against potential risks, a crucial process for ensuring safe peptide use. Outcomes reported in studies can vary in their relevance to clinical practice. Many studies focus on surrogate endpoints - like lab values or biomarker changes - rather than outcomes that directly impact patients, such as reduced symptoms, improved function, or better quality of life. For example, a short-term improvement in a biomarker over four weeks doesn’t guarantee long-term effectiveness or durability.
When reviewing results, look for absolute changes in addition to relative ones. A claim of "50% reduction" might sound impressive, but if the baseline risk was only 2%, the absolute benefit is just 1%. Confidence intervals (CIs) are also important - a wide CI indicates the study may be underpowered, leaving the true effect size unclear. Additionally, examine how adverse events were tracked. Systematic methods provide more reliable data than voluntary reporting, and discontinuation rates can offer valuable insights into tolerability.
| Outcome Type | Example | Clinical Value |
|---|---|---|
| Surrogate endpoint | IGF-1 level increase | Indirect; hypothesis-generating |
| Patient-centered outcome | Improved mobility score | Direct; clinically meaningful |
| Safety signal | Injection-site reaction rate | Essential for benefit-risk assessment |
For peptides that influence growth-promoting pathways - such as those affecting IGF-1 or angiogenesis (e.g., TB-500) - it’s particularly important to check whether the study considered oncology-related risks, even if only in theory.
Applying Research Findings to Patient Care
Staying Aligned With U.S. Regulatory Requirements
Before using a peptide in clinical practice, confirm its regulatory classification - whether it's FDA-approved, compounded, Research Use Only (RUO), or falls into a less-defined category. FDA-approved peptides should always be the first choice. If compounded peptides are under consideration, it’s crucial to note that the FDA has been shifting many peptides from Category 2 to Category 1, which means they can no longer be compounded unless there’s a documented patient-specific need under the 503A exemption process. RUO peptides should never be used for human administration, as they may contain residual solvents that could accumulate in the body over time.
"The future of peptide medicine will likely belong to clinicians who understand three things simultaneously: the science, the regulatory environment, and the ethical responsibility of prescribing intelligently." - Benjamin González, MD, Integrative and Functional Medicine Physician
To ensure compliance, document the following: a valid physician-patient relationship, the clinical justification for selecting a peptide over an FDA-approved alternative, and a clear monitoring plan. Once the peptide's regulatory status is confirmed, its use should be tailored to maximize clinical benefits while addressing patient-specific risks.
Building a Benefit-Risk Framework for Each Patient
Once regulatory guidelines are addressed, the next step is to carefully evaluate the individual patient to ensure that the potential benefits of peptide therapy outweigh the risks. This process involves grounding decisions in evidence directly relevant to the patient’s condition, rather than relying solely on generalized study findings. For instance, peptides like BPC-157 or TB-500, which mainly have animal studies and small pilot trials backing them, carry a different risk profile than FDA-approved peptides supported by Phase III clinical trial data.
Start by identifying hard exclusions. Conditions such as active or recent malignancy, pregnancy, and breastfeeding are absolute contraindications for most peptides, particularly those that affect angiogenesis or cell growth pathways. Drug interactions also need attention. For example, GLP-1 agonists slow gastric emptying, which can interfere with the absorption of medications like oral contraceptives, antibiotics, and anticoagulants such as warfarin.
| Patient Factor | What to Assess |
|---|---|
| Malignancy history | Exclude peptides that stimulate angiogenesis or IGF-1 pathways |
| Co-medications | Monitor for absorption delays, especially with GLP-1 agonists |
| Metabolic baseline | Check IGF-1, fasting glucose, and HbA1c before using GH-axis peptides |
| Immune status | Perform CBC and CMP before starting immune-modulating peptides |
The quality of the peptide is another critical factor. Peptides sourced from unregulated vendors may be contaminated with heavy metals, bacterial endotoxins, or synthesis impurities. To mitigate this risk, only use peptides from 503A or 503B pharmacies that provide third-party Certificates of Analysis (COA) verifying potency, purity, and sterility.
How to Introduce Peptide Therapy Safely
When starting peptide therapy, follow a "start low, go slow" approach. Begin with a conservative dose to monitor tolerance and document the patient’s clinical response. This creates a clear clinical record, which can be invaluable if questions about the treatment arise later.
Baseline laboratory tests - such as IGF-1, fasting glucose, HbA1c, CBC, and CMP - should be completed before initiating therapy. Additionally, informed consent is critical. Patients must be explicitly informed in writing that the peptide is compounded, not FDA-approved, and that there may be limited long-term safety data.
For investigational peptides like BPC-157 or TB-500, limit their use to clearly defined 4–8 week courses, with a reassessment documented at the end of each cycle. This structured approach ensures that therapy remains grounded in clinical reasoning. It also provides a clear decision point to either continue, adjust, or discontinue treatment based on the patient’s actual response.
Tools and Resources to Support Clinical Decision-Making
Using Evidence-Based Clinical Resources
Keeping up with the latest in peptide research can feel overwhelming, but clinical tools can make this process much simpler and help you feel more confident in your prescribing choices. One such resource is PeptidePrescriber, a platform specifically designed for licensed clinicians working in this area. It provides evidence-based peptide monographs along with practical tools like reconstitution and unit conversion calculators, dosing protocols, injection guides, and regulatory references. Importantly, it remains pharmacy-agnostic, offering unbiased guidance no matter which compounding vendor you use. While the reconstitution and unit conversion tools are free for public use, the full clinical library - complete with editable consent templates and a regulatory quick reference - is part of the platform's Starter Pack.
"The evidence grading alone is worth it. I can tell patients exactly where the science stands instead of guessing." - Dr. James R., Sports Medicine
When evaluating peptide claims, it's crucial to verify information using reliable sources like PubMed IDs (PMIDs) or DOIs, rather than relying solely on summaries or marketing materials. These secondary sources can serve as a helpful introduction but shouldn't replace primary research. Alongside digital tools, engaging in ongoing discussions with peers is another key to staying informed.
Learning From Peers and Ongoing Education
While structured tools are invaluable, insights from colleagues can add another layer of depth to your clinical decision-making. Peptide science is constantly evolving, and no single resource can cover everything. For example, regulatory classifications are shifting - starting in March 2024, the FDA began reclassifying peptides from Category 2 to Category 1. Staying informed requires more than just occasional literature searches. Peer networks allow clinicians to share dosing experiences, flag potential safety concerns, and discuss adjustments for unique cases that aren't always addressed in published studies.
PeptidePrescriber also includes a prescriber network, connecting clinicians actively working with peptide therapies. For more formal education, organizations like the American Academy of Anti-Aging Medicine (A4M) offer structured CME opportunities, providing a framework for peer-led learning. By combining digital tools with peer exchanges, clinicians can apply peptides more safely and effectively, gaining a comprehensive understanding of where the science is today and where it’s headed tomorrow.
Conclusion: Integrating Peptides Into Practice Responsibly
When it comes to integrating peptides into clinical practice, responsibility starts with a commitment to evidence-based care. Safe prescribing hinges on solid research, staying updated on regulations, and prioritizing patient safety. Always evaluate the peptide's level of clinical evidence and confirm its regulatory status before proceeding.
Before initiating peptide therapy, take these crucial steps: verify FDA approval, assess the peptide's evidence base, review the patient’s medical history (especially for conditions like malignancy), and use a peptide prescriber starter pack to ensure the peptide is sourced from a licensed 503A or 503B pharmacy with a valid third-party Certificate of Analysis. These measures help establish a defensible, patient-centered practice that minimizes risks.
Patient safety and thorough documentation should remain central to every peptide-related decision. For compounded or off-label peptides, it’s essential to inform patients about the experimental nature of the treatment and the limited data on long-term safety. Documenting these discussions is critical, as standard malpractice insurance often excludes coverage for claims involving unapproved drugs.
The regulatory environment surrounding peptides is constantly shifting. FDA reclassifications, state enforcement actions, and changes in compounding guidelines mean that what’s allowed today may not be tomorrow. Staying informed, verifying sources, and applying sound clinical judgment are necessary steps to protect both patients and yourself. By keeping your knowledge current and relying on evidence-based tools, you can confidently and responsibly incorporate peptide therapy into your practice.
For further guidance, including regulatory updates and dosing tools mentioned throughout this guide, healthcare professionals can access resources at PeptidePrescriber.
FAQs
How can I tell if a peptide has enough human evidence to use clinically?
When determining whether a peptide is ready for clinical use, prioritize randomized, controlled human trials. These provide stronger evidence compared to preclinical data like animal studies or anecdotal reports. Here's a breakdown of evidence tiers to guide your assessment:
- Approved Drugs: Backed by FDA or similar regulatory approvals.
- Clinical Trials: Includes human Phase I/II trials that provide early insights into safety and effectiveness.
- Pilot Data: Based on smaller studies or case series, offering preliminary findings.
- Preclinical Only: Limited to research on animals or cell models, lacking human data.
PeptidePrescriber offers tools and resources to help you evaluate the evidence and ensure peptides are applied safely in clinical settings.
What should I document to stay compliant when prescribing compounded peptides?
To ensure compliance, it's crucial to document a valid physician-patient relationship that has been established during a clinical encounter. This should include a detailed history and physical exam. Clearly outline the medical necessity for the treatment and explain why standard therapies were not appropriate for the patient's condition.
Make sure to obtain and thoroughly document informed consent from the patient. Keep comprehensive records of your clinical reasoning, monitoring strategies, and follow-up plans. Additionally, confirm that your pharmacy is properly licensed and strictly follows FDA regulations for compounding.
How do I spot safety red flags in peptide studies before treating patients?
When evaluating peptide studies, it's crucial to dig into the study's design. Here’s what to watch out for:
- No control groups or human trials: Research that skips these steps doesn’t provide enough evidence to draw reliable conclusions.
- Animal model findings applied to humans: Be cautious. Results from animal studies don’t always translate to human outcomes.
For products, insist on a Certificate of Analysis (COA). A COA ensures the product has been tested for quality and safety. Be alert for these warning signs:
- Missing lot numbers
- Lack of third-party testing
- Presence of contaminants like bacterial endotoxins
Also, avoid peptides labeled as “for research use only.” These products fall outside regulatory oversight, making their safety and efficacy uncertain.
If you're navigating clinical practice, tools like PeptidePrescriber can help you make safer, more informed decisions.