
Peptide therapy offers targeted solutions for managing metabolic conditions like obesity, type 2 diabetes, and metabolic syndrome. Unlike traditional treatments that focus on symptoms, peptides address root causes such as insulin resistance, hormone signaling, and fat metabolism. Key peptides like GLP-1 receptor agonists (e.g., semaglutide), growth hormone secretagogues (e.g., tesamorelin), and tissue-repair peptides (e.g., BPC-157) are central to effective protocols.
Key Takeaways:
- Who Benefits? Patients with obesity (BMI ≥30 or ≥27 with comorbidities), prediabetes, type 2 diabetes, or metabolic syndrome.
- How It Works: Peptides regulate appetite, improve insulin sensitivity, reduce visceral fat, and preserve lean muscle.
- Combination Therapy: Pairing GLP-1 agonists with growth hormone secretagogues enhances results, managing appetite while maintaining muscle mass.
- Monitoring: Regular lab work (e.g., HbA1c, IGF-1) and tracking metrics like weight and body composition ensure safety and effectiveness.
- Dosing: Start low and titrate gradually to minimize side effects like nausea or gastrointestinal discomfort.
This guide outlines the step-by-step process for selecting peptides, dosing, monitoring, and managing risks to create tailored, physician-guided protocols.
Peptide Stacking 101: Safely Combine Peptides and GLP-1s
sbb-itb-7164bd9
Identifying Metabolic Patients Who Are Good Candidates for Peptide Therapy
Not every patient with a metabolic condition is suited for peptide therapy. The key to success lies in selecting the right candidates upfront - this ensures effective treatments while minimizing unnecessary risks. Accurate identification is the first step in creating tailored protocols, as discussed later.
Understanding Metabolic Phenotypes
Patients who may benefit from peptide therapy typically fall into four categories: obesity, prediabetes, type 2 diabetes (T2DM), and metabolic syndrome. Each group has specific markers that guide eligibility and peptide selection.
For obesity, eligibility begins with a BMI of ≥30 kg/m² or ≥27 kg/m² if accompanied by conditions like hypertension, dyslipidemia, or sleep apnea. Waist circumference also plays a role since increased visceral fat can lead to insulin resistance, even in patients with borderline BMIs. Prediabetes and T2DM are identified through markers like fasting glucose, HbA1c, and HOMA-IR (calculated as fasting glucose × fasting insulin ÷ 405). A HOMA-IR score above 2.9 often indicates the need for metabolic intervention.
For example, the SCALE Prediabetes trial found that 66.2% of participants on liraglutide reverted to normoglycemia, compared to 36% on placebo after 160 weeks. This highlights the potential of peptide therapy in addressing early metabolic dysfunction.
Inclusion and Exclusion Criteria
The table below outlines how specific peptide classes align with particular phenotypes, alongside eligibility markers and contraindications:
| Peptide Class | Phenotype | Key Eligibility Markers | Major Contraindications |
|---|---|---|---|
| GLP-1 RAs (e.g., Semaglutide) | Obesity, T2DM, Prediabetes | BMI ≥27–30, A1C >5.7%, Fasting Glucose | MTC, MEN 2, Pancreatitis, Pregnancy |
| Dual Agonists (e.g., Tirzepatide) | Severe Obesity, Metabolic Syndrome | BMI >35, HOMA-IR >2.9, High Visceral Fat | MTC, MEN 2, Pancreatitis, Hypersensitivity |
| GHRH Analogs (e.g., Tesamorelin) | Visceral Adiposity, HIV Lipodystrophy | Waist Circumference, Liver Fat Fraction | Active Malignancy, Pregnancy |
| GH Secretagogues (e.g., Ipamorelin) | Sarcopenic Obesity, Body Recomposition | Lean Mass %, IGF-1 Levels | Active Malignancy |
Patients with a personal or family history of medullary thyroid carcinoma (MTC) or multiple endocrine neoplasia type 2 (MEN 2) should avoid GLP-1 and dual agonist therapies. Other contraindications include pancreatitis, severe gastrointestinal conditions like gastroparesis or IBD, active eating disorders, and pregnancy or breastfeeding. Growth hormone secretagogues are not recommended for patients with active malignancies due to potential proliferative risks. Additionally, combining GLP-1 therapies with insulin or sulfonylureas may increase hypoglycemia risk, necessitating careful dose adjustments.
"The recognition of obesity as a chronic disease requiring medical management has fundamentally shifted treatment paradigms from short-term interventions to comprehensive, long-term treatment approaches." - StatPearls
Once eligibility is confirmed and contraindications are addressed, document baseline clinical markers to guide future treatment.
Baseline Assessments and Documentation
After identifying suitable candidates, a structured baseline evaluation ensures eligibility and sets up monitoring protocols. This includes a comprehensive lab panel and physical assessments to establish starting points for treatment.
| Assessment Category | Required Tests | Clinical Purpose |
|---|---|---|
| Glycemic Status | HbA1c, Fasting Glucose | Identifies prediabetes/T2DM and tracks improvement |
| Organ Function | CMP (Creatinine, eGFR, ALT, AST) | Evaluates kidney and liver function; flags dehydration risk |
| Cardiovascular | Lipid Panel (Triglycerides, LDL) | Assesses cardiovascular risk and pancreatitis markers |
| Endocrine Safety | TSH, Thyroid History | Screens for thyroid dysfunction and contraindications |
| Pancreatic Health | Lipase, Amylase | Reviews history of pancreatitis or abdominal pain |
| Insulin Resistance | Fasting Insulin, HOMA-IR, C-peptide | Quantifies insulin resistance and predicts therapy response |
Baseline lab panels from direct-to-consumer services typically cost $130 to $160 (USD) as of 2026, making them accessible for cash-pay patients. Physical evaluations should include BMI, waist circumference, blood pressure, and heart rate at every visit. For women of childbearing age, a urine or serum hCG test is mandatory before starting therapies like GLP-1 or GIP. If growth hormone peptides are part of the plan, baseline IGF-1 levels must be documented.
U.S. clinical guidelines also require a detailed intake history, including family thyroid tumor history, and documentation of all baseline labs before prescribing. For compounded peptides, ensure that the pharmacy complies with compounded peptide regulations and USP <797> sterile compounding standards to protect patient safety and reduce liability. These baseline steps set the stage for the monitoring and adjustments covered in later sections.
Key Peptides Used in Metabolic Therapy
When starting metabolic therapy, the focus often lands on three main peptides: GLP-1 receptor agonists, growth hormone secretagogues, and tissue-healing peptides like BPC-157. These peptides serve as the foundation for the dosing and selection strategies outlined in later sections.
GLP-1 Receptor Agonists
GLP-1 receptor agonists work by mimicking glucagon-like peptide-1, a hormone that helps regulate blood sugar. They stimulate insulin release when blood sugar levels are high, reduce glucagon production, slow gastric emptying, and promote a feeling of fullness. Clinical trials have shown impressive results. For example, in the STEP 1 trial, adults with a BMI of 30 or higher who took 2.4 mg of semaglutide weekly alongside lifestyle changes lost an average of 14.9% of their body weight over 68 weeks, compared to just 2.4% in the placebo group. Beyond weight loss, these agents typically lower HbA1c by about 1% and even offer cardiovascular benefits. In fact, semaglutide reduced major cardiovascular events by 20% over five years.
"GLP-1 receptor agonists have also demonstrated the ability to restore insulin secretory functions, thereby improving glycemic control and body weight reduction in diabetic patients." - StatPearls
These medications are available in daily injectable forms like liraglutide or weekly options such as semaglutide and dulaglutide. A newer option, tirzepatide, has shown even greater potential. A 15 mg weekly dose reduced HbA1c by 2.34% and body weight by 10.5 kg over 40 weeks. Emerging triple agonists, which target GLP-1, GIP, and glucagon receptors, have shown an average weight loss of 22% in Phase II trials over 48 weeks. Common side effects include nausea and vomiting, and these drugs are not recommended for individuals with a personal or family history of medullary thyroid carcinoma.
Growth Hormone Secretagogues
Growth hormone secretagogues (GHS) stimulate the pituitary gland to release growth hormone (GH) in a natural, pulsatile manner. This results in increased levels of IGF-1, which helps reduce visceral fat, build lean muscle, and improve bone density.
These secretagogues fall into two main categories. First, GHRH analogs like Tesamorelin and CJC-1295 enhance the body’s natural GH pulses. Tesamorelin, for instance, is FDA-approved for reducing visceral fat in HIV-associated lipodystrophy. Second, GH-releasing peptides (GHRPs) like Ipamorelin act by mimicking ghrelin to trigger GH release. Ipamorelin is particularly notable because it avoids significant cortisol spikes, unlike earlier GHRPs such as GHRP-2 or GHRP-6. For those who prefer oral options, MK-677 (Ibutamoren) offers sustained GH and IGF-1 elevation for about 24 hours with a once-daily dose, though it may increase the risk of insulin resistance in some cases.
It’s important to monitor fasting glucose and HbA1c levels, as non-selective GHRPs can increase cortisol and prolactin levels.
BPC-157 and Other Tissue-Healing Peptides
BPC-157, a 15-amino-acid peptide derived from human gastric juice, is primarily known for its tissue-repair capabilities. It promotes healing by enhancing VEGF-driven angiogenesis and activating pathways that help cells migrate. In metabolic therapy, BPC-157 is mainly used to address gastrointestinal side effects caused by GLP-1 treatments, such as nausea, bloating, and acid reflux due to delayed gastric emptying. For example, in the STEP 1 semaglutide trial, 44% of participants reported nausea, highlighting the need for supportive measures.
BPC-157 is typically introduced after establishing a baseline with GLP-1 therapy to better attribute any side effects. Oral doses (100–500 mcg once or twice daily) are favored for gastrointestinal support, while subcutaneous injections (150–375 mcg twice daily) are used for broader tissue repair.
Regulatory changes are also worth noting. As of April 22, 2026, the FDA has removed BPC-157 from the Category 2 bulk drug substances list, meaning it can no longer be compounded by standard 503A pharmacies. Physicians must now ensure that compounding pharmacies operate under a compliant 503B framework. BPC-157 is contraindicated in cases of active malignancy or proliferative retinopathy.
Understanding the role of these peptides is essential for creating a well-rounded and effective metabolic therapy protocol.
How to Build a Peptide Protocol for Metabolic Patients Step by Step
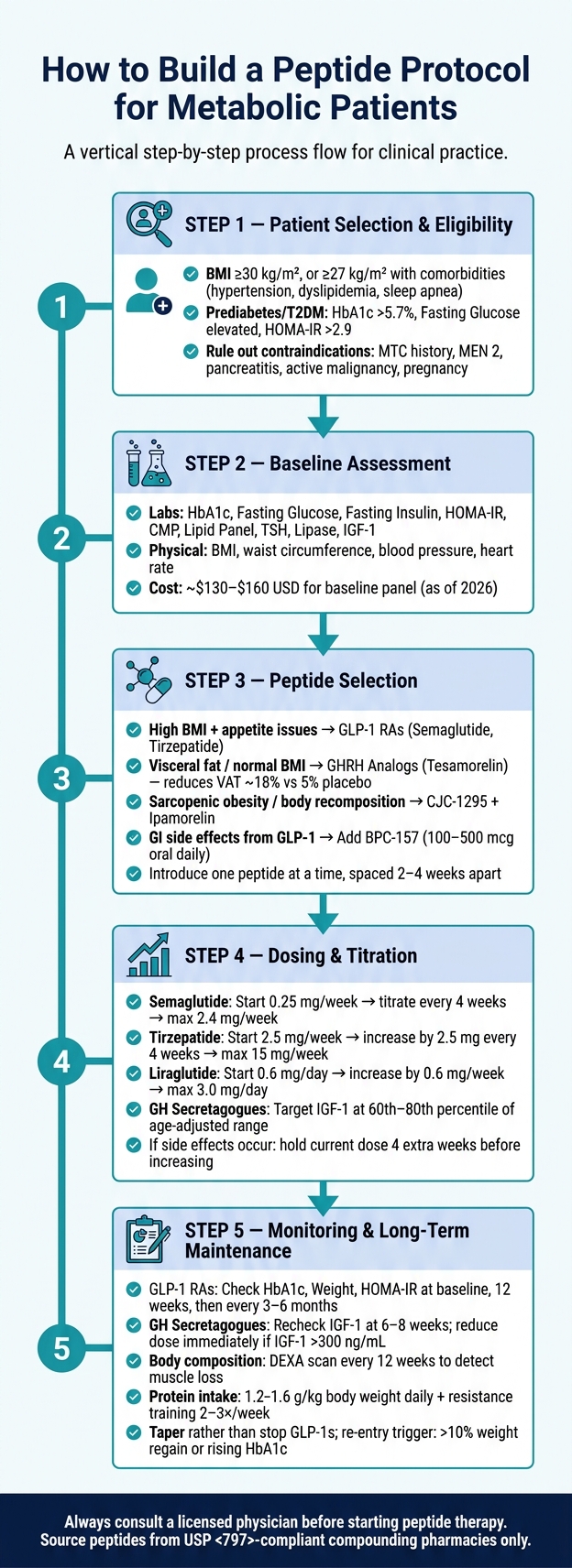
Step-by-Step Peptide Protocol for Metabolic Patients
Choosing the Right Peptide or Combination
The first step in creating a peptide protocol is tailoring the choice of peptides to the patient's specific metabolic profile. For example, patients with a high BMI and appetite regulation challenges may benefit from GLP-1 receptor agonists like semaglutide or tirzepatide. On the other hand, patients with a normal BMI but increased visceral adipose tissue (VAT) might respond better to Tesamorelin, which has been shown to reduce VAT by around 18%, compared to just 5% in placebo groups. For those prioritizing body recomposition and lean mass preservation, CJC-1295 paired with Ipamorelin can be a good fit.
Combination therapy is becoming a standard approach, as metabolic dysfunction often involves multiple pathways. For instance, pairing GLP-1 agonists with GH secretagogues can help manage appetite while preserving muscle mass. This is particularly important given that lean soft tissue can account for 26–40% of the total weight lost during GLP-1 therapy. To minimize risks and pinpoint any side effects, introduce one peptide at a time, spacing each addition by 2–4 weeks.
This thoughtful selection process lays the groundwork for effective dosing and sustainable metabolic management.
Dosing and Titration Strategies
After selecting the most appropriate peptide or combination, the next step is to determine the right dosing and titration strategy. The key is to prioritize tolerance over speed, especially with GLP-1 therapies, where gastrointestinal side effects are common during the first 1–8 weeks of treatment.
Here’s a quick guide to starting doses and titration schedules:
| Peptide | Starting Dose | Titration Schedule | Maximum Dose |
|---|---|---|---|
| Semaglutide (Ozempic/Wegovy) | 0.25 mg weekly | Increase every 4 weeks (0.25 → 0.5 → 1.0 → 2.0/2.4 mg) | 2.4 mg weekly |
| Tirzepatide (Mounjaro/Zepbound) | 2.5 mg weekly | Increase by 2.5 mg every 4 weeks | 15 mg weekly |
| Liraglutide (Saxenda) | 0.6 mg daily | Increase by 0.6 mg weekly | 3.0 mg daily |
The FDA label for Ozempic notes that "The 0.25 mg dosage is intended for treatment initiation and is not effective for glycemic control". If side effects occur when increasing the dose, it’s better to maintain the current dose for an extra 4 weeks before attempting further titration. For GH secretagogues, aim to keep IGF-1 levels within the 60th to 80th percentile of the age-adjusted range. This avoids pushing levels too close to the upper limit, maintaining a safer therapeutic window.
Administration Methods and Protocol Duration
Once the dosing is optimized, proper administration and a defined protocol duration are crucial for achieving the desired results. Subcutaneous (SC) injection is the go-to method for peptides like GLP-1 agonists and GH secretagogues. To prevent localized reactions, rotate injection sites weekly. Administering these injections at bedtime can also help patients sleep through any nausea that might occur after a new or increased dose.
The length of the protocol depends on the peptide being used and the patient’s goals. GLP-1 therapies often require long-term use since stopping treatment can lead to regaining 60–70% of the lost weight within a year. It’s important to set clear cessation criteria based on clinical benchmarks rather than patient preference alone. Alongside the peptide protocol, lifestyle adjustments are essential. Patients should aim to consume 1.2–1.6 g of protein per kilogram of body weight daily and engage in resistance training 2–3 times a week to help preserve lean mass.
"The framework that produces durable results is one where a peptide addresses the upstream signaling defect while lifestyle change rebuilds the tissue-level infrastructure." - Meto Editorial Team
Monitoring Progress, Adjusting Protocols, and Managing Risks
Monitoring Metrics and Lab Work
Once a peptide protocol is in place, consistent monitoring becomes critical to ensure safety and effectiveness. The key is to focus on trends rather than isolated data points. For example, a single elevated result is less meaningful than observing patterns over time.
For GLP-1 therapies, the primary markers to track are HbA1c, fasting glucose, and HOMA-IR (calculated as fasting glucose × fasting insulin ÷ 405). When it comes to GH secretagogues, IGF-1 is the most important metric:
"IGF-1 is the single most informative number you own... every serious protocol titrates to an IGF-1 target, not to a milligram dose." - FormBlends
To ensure accuracy, blood draws should be scheduled between 7:00 AM and 10:00 AM after a proper 10–12 hour fast (water only). Patients should stop taking biotin supplements at least 72 hours prior, as biotin can interfere with hormone and thyroid test results.
| Peptide Class | Efficacy Marker | Safety Markers | Monitoring Frequency |
|---|---|---|---|
| GLP-1 RAs | HbA1c, Weight, HOMA-IR | Creatinine, eGFR, Lipase (if symptomatic) | Baseline, 12 weeks, then every 3–6 months |
| GH Secretagogues | IGF-1, IGFBP-3 | Fasting Glucose, HbA1c, Prolactin | Baseline, 6–8 weeks, 12 weeks, then every 3–6 months |
| Tissue Repair (BPC-157) | Functional outcomes (Pain/ROM) | CMP (Liver function), CBC | Baseline, 4–6 week follow-up |
For GH secretagogues, an IGF-1 recheck at 6–8 weeks is essential, as levels typically stabilize around this time. If IGF-1 exceeds 300 ng/mL, the dose should be reduced immediately.
Once metrics are tracked, attention turns to managing potential side effects effectively.
Managing Adverse Effects
Side effects are a common concern, especially with metabolic peptide protocols. For GLP-1 therapies, nausea, diarrhea, and vomiting are reported by 20–40% of users, with tirzepatide users experiencing rates as high as 66%. If nausea persists beyond two weeks at a new dose, it’s often best to maintain that dose for an additional four weeks before increasing.
Certain findings, however, demand immediate action:
| Finding | Required Action |
|---|---|
| ALT or AST > 5× upper limit | Stop all peptides; seek clinical evaluation |
| Lipase > 3× upper limit + abdominal pain | Stop GLP-1s immediately; evaluate for acute pancreatitis |
| eGFR drop >25% from baseline | Stop therapy, hydrate, and evaluate immediately |
| IGF-1 > 300 ng/mL (adults) | Immediate dose reduction |
| Fasting glucose rise > 25 mg/dL | Reassess protocol; recheck HbA1c |
For patients on tirzepatide, it’s important to advise using non-oral contraceptive methods for four weeks after starting or increasing the dose, as delayed gastric emptying can reduce the effectiveness of oral birth control. If GLP-1 therapy is interrupted for more than two weeks, always restart at the lowest initial dose - such as 0.25 mg weekly for semaglutide - to minimize the risk of rebound gastrointestinal issues or pancreatitis.
Addressing side effects is just one part of the equation. Long-term strategies are essential for maintaining progress.
Long-Term Maintenance and Relapse Prevention
For long-term success, reducing doses rather than stopping therapy altogether often yields better results. GLP-1 doses may be tapered to the lowest level that maintains weight stability. Alongside this, encourage patients to consume 1.2–1.6 g of protein per kilogram of body weight daily and engage in resistance training 2–3 times a week to preserve lean muscle mass. Regular body composition checks using DEXA scans every 12 weeks can help detect muscle loss early, allowing for timely adjustments.
"If we helped millions of people lose weight while quietly depleting their muscle mass, the longevity math may not be as favorable as the headline numbers suggest." - Hillary Lin, MD
For patients discontinuing therapy, it’s helpful to establish clear criteria for resuming treatment. For example, re-entry could be triggered by regaining more than 10% of lost body weight or a noticeable rise in HbA1c. This ensures decisions are guided by clinical need rather than reactive measures.
Conclusion: Building Safe and Effective Peptide Protocols for Metabolic Patients
Creating effective peptide protocols begins with a detailed baseline assessment and concludes with a well-defined plan for long-term care. At every stage, clinical expertise is essential.
Patient selection is critical. For example, screening for contraindications like a history of medullary thyroid carcinoma before starting GLP-1 therapy or ruling out active malignancy before prescribing GH secretagogues isn't optional - it’s essential. As Dr. Jerath succinctly stated: "Starting peptide therapy without lab testing removes the safety guardrails that make the treatment work."
Using peptides from reputable, licensed compounding pharmacies that adhere to USP <797> and <795> standards is another non-negotiable. These pharmacies provide Certificates of Analysis, ensuring the quality and consistency of their products. On the other hand, independent assays of unregulated online peptides have revealed discrepancies in concentrations ranging from 30% to 90% compared to their labels. This stark variability highlights the risks of using substandard products and the importance of sourcing only verified peptides.
The most effective protocols rely on multi-mechanism approaches combined with careful dose adjustments. For example, pairing a GLP-1 for appetite control with a GH secretagogue for muscle preservation, starting at the lowest effective dose, and gradually increasing every four weeks offers a balanced strategy. This method not only promotes fat loss but also helps maintain lean muscle mass. Additionally, tools like DEXA scans - rather than just tracking scale weight - are essential for distinguishing true body recomposition from basic weight loss.
"Peptides provide surgical precision in metabolic signaling, allowing clinicians to shift focus from mere weight loss to true body composition optimization." - Cellgenic
The success and safety of peptide therapy hinge on a structured approach: comprehensive baseline labs, evidence-based peptide selection, gradual titration, regular monitoring, and clear criteria for adjusting or discontinuing treatment. This systematic process is what elevates peptide therapy from a simple intervention to a precise medical practice.
FAQs
What’s the safest first peptide to start with?
GLP-1 receptor agonists are a popular choice because they come with a wealth of clinical trial data and have FDA approval. These medications are often prescribed for improving metabolic health and assisting with weight management. When it comes to optimizing growth hormone levels, Sermorelin is frequently selected thanks to its safety profile and its role in supporting the body’s natural hormone production. It's crucial to start with a thorough clinical evaluation, including baseline lab work, to ensure the treatment is safe and to identify any potential contraindications.
Which labs matter most before and during treatment?
Lab testing plays an essential role in ensuring safety, spotting potential issues, and keeping track of progress when following metabolic protocols. A standard baseline panel often includes a Comprehensive Metabolic Panel (CMP), Complete Blood Count (CBC), lipid panel, and HbA1c. It’s also important to measure fasting glucose, fasting insulin (using HOMA-IR), and TSH to assess thyroid function.
For those using GLP-1 agonists, regular monitoring of HbA1c, CMP, and lipid levels every 90 days is recommended. When it comes to GH-axis peptides, keeping an eye on IGF-1 levels helps guide dosing and ongoing monitoring.
How do you prevent muscle loss on GLP-1s?
To help maintain muscle while undergoing GLP-1 therapy, it's important to pair thoughtful nutrition with a consistent exercise routine. Aim to consume 1.2–1.6 grams of protein per kilogram of body weight each day, evenly distributed across 3–4 meals. Include full-body resistance training sessions 2–3 times per week to preserve muscle mass. For added support, consider taking 3–5 grams of creatine monohydrate daily, which may aid in retaining muscle and boosting strength.