Here’s the short answer: liraglutide may help muscle move more GLUT4 to the cell surface, but most of that evidence comes from cell and animal studies, not direct human muscle studies.
If you want the takeaway fast, it’s this:
- Acute preclinical studies show liraglutide can increase AMPK, AS160/TBC1D4, and TBC1D1 signaling and shift existing GLUT4 to the muscle cell membrane.
- Chronic cell studies are mixed. In some healthy-muscle models, liraglutide did not increase membrane GLUT4 or basal glucose uptake.
- Insulin-resistant models show the clearest effect, with repair of impaired signaling, more GLUT4 expression, and better glucose handling.
- Animal data suggest better muscle glucose use and possible glycogen storage, but human muscle biopsy data are still scarce.
- So, for me, the safest read is simple: this is useful mechanism, not proof of a direct human muscle-glycogen effect.
A few numbers help frame it:
- In L6 myotubes, liraglutide was linked to about a 70% increase in TBC1D1 phosphorylation.
- In high-fat diet rats, insulin-stimulated glucose disposal went from 3.67 ± 0.34 to 4.95 ± 0.31 mg·kg⁻¹·min⁻¹, or about 35% higher during clamp testing.
- In diabetic rodent studies, liraglutide increased skeletal muscle Slc2a4 mRNA, GLUT4 protein, and some glycolytic enzyme activity.
If I were explaining this clinical overview to a clinician in one line, I’d say: liraglutide may help insulin-resistant muscle handle glucose better, but the case for direct human muscle GLUT4 or glycogen effects is still incomplete.
That’s the lens I’d use for the rest of this review: focus on what the data show, where they came from, and where the human gap still sits. This gap underscores the importance of rigorous patient selection criteria when considering these therapies.
Pathways: How Liraglutide May Increase Muscle GLUT4 Translocation
Baseline: Canonical Insulin Signaling and GLUT4 Trafficking
In skeletal muscle, insulin signaling follows a familiar route: the insulin receptor, then IRS-1/2, PI3K, Akt2, and after that AS160/TBC1D4 and TBC1D1. That chain lets GLUT4 vesicles move to the cell membrane. In muscle, TBC1D1 stands out because it is more abundant than AS160 and can also be phosphorylated by AMPK.
AMPK, cAMP, AS160, and TBC1D1 in Liraglutide-Treated Myotubes
With that baseline in mind, liraglutide seems to work mainly through AMPK-linked GLUT4 trafficking in preclinical muscle models. In C2C12-GLUT4myc myotubes, acute liraglutide increased cAMP, activated AMPK, phosphorylated AS160/TBC1D4 and TBC1D1, and moved GLUT4 to the sarcolemma without increasing total GLUT4.
Context matters here. Acute exposure and insulin-resistant cells do not behave the same way.
In L6 myotubes, liraglutide increased glucose uptake through AMPK activation and TBC1D1 phosphorylation, with about a 70% increase in TBC1D1 phosphorylation. In palmitate-exposed L6 myotubes, liraglutide increased SESN2, restored p-Akt/Akt signaling, and increased GLUT4 protein expression. When autophagy was blocked, those gains were blunted.
Put simply, the main acute signal looks like AMPK-driven GLUT4 movement. By contrast, SESN2/Akt-linked effects seem more tied to insulin-resistant muscle.
Akt and Autophagy-Linked Effects in Insulin-Resistant Muscle Models
The preclinical literature points to two main patterns:
| Pathway | Key proteins | Liraglutide's apparent role | Evidence context |
|---|---|---|---|
| AMPK-linked (acute) | GLP-1R, cAMP, AMPK, AS160/TBC1D4, TBC1D1, GLUT4 | Increases phosphorylation and redistributes existing GLUT4 pools | C2C12 and L6 myotubes, acute exposure |
| SESN2/Akt/autophagy | SESN2, p-Akt/Akt, GLUT4 | Restores impaired signaling and supports GLUT4 expression | Palmitate-exposed L6 myotubes |
The next step is figuring out whether these signaling shifts hold up with longer exposure and in tissue-level models.
sbb-itb-7164bd9
Study Models and Dosing Context From the Literature
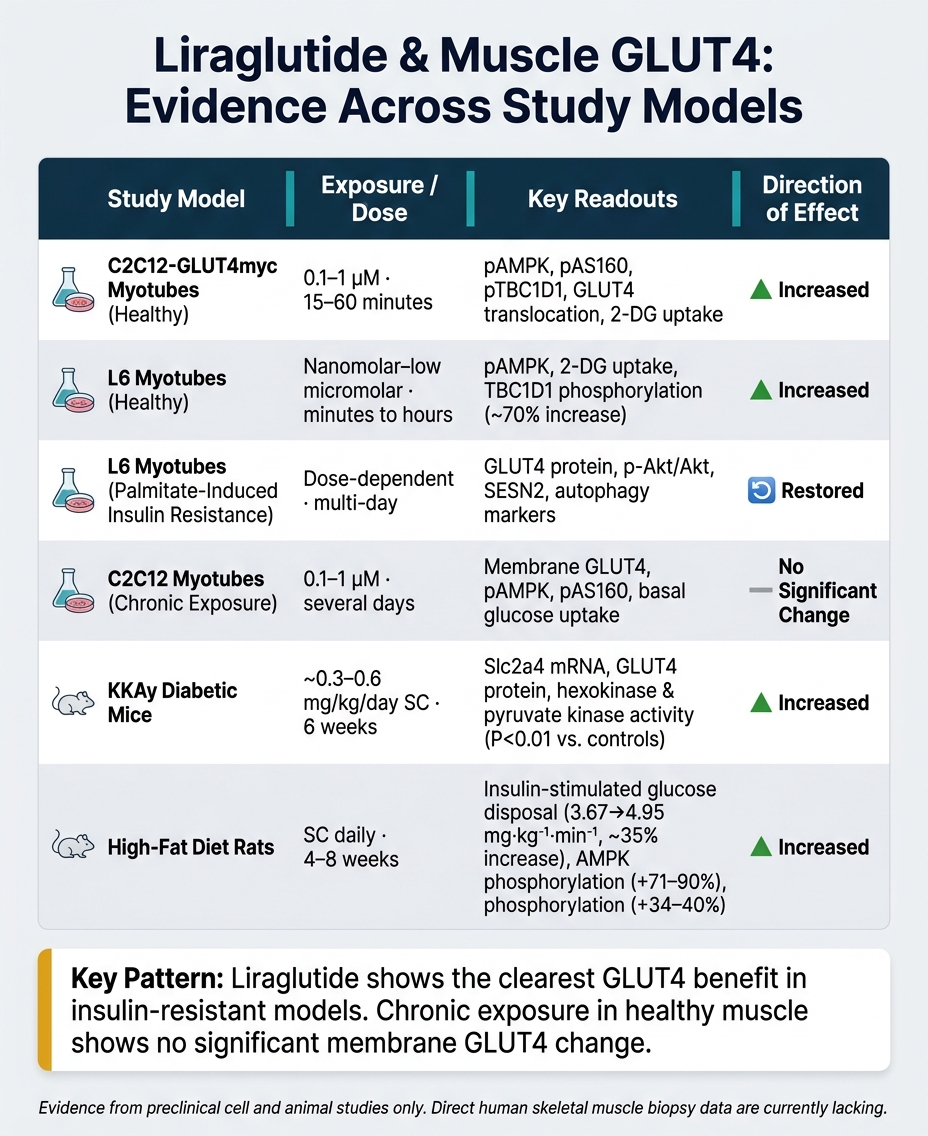
Liraglutide & Muscle GLUT4: Preclinical Evidence Across Study Models
Acute In Vitro Exposure: Early Signaling and GLUT4 Movement
The next thing to sort out is simple: do these signaling effects stick around with longer exposure and in living organisms, or do they fade once the first burst is over?
Short-term cell work gives the clearest mechanistic signal for liraglutide-driven GLUT4 movement. In C2C12-GLUT4myc myotubes, liraglutide at 0.1 to 1 µM for 15 to 60 minutes increased cAMP and AMPK-linked GLUT4 movement. In L6 rat myotubes, short exposure also increased AMPK phosphorylation and 2-deoxyglucose (2-DG) uptake in an insulin-independent way.
That said, there’s an obvious catch. These doses are above what humans usually see in clinical use, and the cell-culture setup doesn’t mirror the metabolic state of someone with diabetes. So the acute signal is useful for mechanism, but it doesn’t settle the clinical question. For more clinical insights on peptide therapy, staying current with evidence-based research is essential.
Chronic Exposure: Mixed Findings on Membrane GLUT4 and Glucose Uptake
Once exposure lasts longer, the picture gets messier.
A recent study in C2C12 cells found that chronic liraglutide treatment did not increase membrane-bound GLUT4, pAMPK/AMPK, pAS160/AS160, or basal glucose uptake versus untreated controls. In plain terms, the early acute effect did not carry over into chronic exposure in that model.
Why the mismatch? Most likely, receptor adaptation plays a part, and model choice matters a lot. In palmitate-induced insulin-resistant L6 cells, liraglutide restored GLUT4, p-Akt/Akt, and SESN2-linked autophagy. That points to an important distinction: liraglutide may work better as a repair tool in impaired signaling states than as a way to push GLUT4 above normal baseline levels.
The readout also changes what you see. Membrane GLUT4, basal glucose uptake, and signaling markers don’t always line up neatly, which is why animal studies matter here. They test whether these cell-level effects show up in actual muscle tissue.
Rodent Dosing and Tissue-Level Outcomes
Animal studies sit in the middle ground between isolated cell signaling and whole-muscle function.
Most rodent studies use subcutaneous liraglutide once or twice daily at 0.3 to 1.0 mg/kg/day for 4 to 8 weeks. On a mg/kg basis, that’s higher than human dosing, but it fits standard preclinical scaling.
In diabetic KKAy mice treated for 6 weeks, liraglutide significantly increased Slc2a4 mRNA and GLUT4 protein in skeletal muscle (P < 0.01 vs. saline-treated diabetic controls). It also increased skeletal muscle hexokinase and pyruvate kinase activities (P < 0.05). Another KKAy mouse study tied liraglutide to PTP1B downregulation, PI3K upregulation, and a significant increase in the p-Akt2/Akt2 ratio (P < 0.01), along with improved muscle ultrastructure.
| Model | Exposure | Main Readouts | Direction |
|---|---|---|---|
| C2C12-GLUT4myc myotubes | 0.1–1 µM, 15–60 min | pAMPK, pAS160, pTBC1D1, GLUT4 translocation, 2-DG uptake | Increased |
| L6 myotubes | Nanomolar to low micromolar, minutes to hours | pAMPK, 2-DG uptake | Increased |
| L6 myotubes (palmitate-induced insulin resistance) | Dose-dependent, multi-day | GLUT4 protein, p-Akt/Akt, SESN2, autophagy | Restored |
| C2C12 myotubes (chronic) | 0.1–1 µM, several days | Membrane GLUT4, pAMPK, pAS160, glucose uptake | No significant change |
| KKAy diabetic mice | ~0.3–0.6 mg/kg/day SC, 6 weeks | Slc2a4 mRNA, GLUT4 protein, HK/PK activity | Increased |
| Diabetic mice (PI3K/Akt2 study) | SC, weeks | PTP1B, PI3K, GLUT4 protein, p-Akt2/Akt2 | Improved |
These model differences matter because membrane GLUT4, glucose uptake, and glycogen repletion do not move in lockstep.
What These Findings Mean for Glucose Uptake and Glycogen Repletion
Expected Effects on Muscle Glucose Uptake
If liraglutide moves GLUT4 to the membrane, the next step is pretty simple: does more glucose actually get into muscle? In plain terms, when more GLUT4 reaches the sarcolemma, skeletal muscle has more doors open for glucose to enter.
The clearest signal shows up in insulin-resistant muscle, not in muscle that already handles glucose well. In high-fat diet rats, liraglutide increased insulin-stimulated glucose disposal by about 35% - from 3.67 ± 0.34 to 4.95 ± 0.31 mg·kg⁻¹·min⁻¹ during euglycemic clamp testing - along with 71–90% higher AMPK phosphorylation and 34–40% higher Akt phosphorylation in skeletal muscle. That matters because it points to a specific pattern: liraglutide seems more likely to help impaired muscle glucose handling than to push normal uptake past baseline. So this is a context-dependent effect, not something seen across the board.
Glycogen Repletion: Plausible but Not Fully Proven
Getting glucose into muscle is only part of the story. The next question is whether that glucose is stored as glycogen, because that’s where the finding starts to matter more in day-to-day physiology. More glucose inside the cell gives the muscle raw material for glycogen synthesis, but storage still depends on insulin signaling, glycogen synthase activity, and when carbohydrate is eaten.
In diabetic KKAy mice, liraglutide increased skeletal muscle GLUT4 expression and was linked with higher glycogen content than in untreated diabetic controls. Exercise research lines up with this idea: higher muscle GLUT4 tends to track with faster glycogen resynthesis. That makes better glycogen repletion plausible, but it still doesn’t make it proven.
There’s also a wrinkle here. In mouse myotubes, chronic liraglutide exposure increased muscle glycogen phosphorylase - an enzyme tied to glycogen breakdown - without increasing membrane GLUT4 or glucose uptake. In other words, the glycogen picture is mixed and depends on the model. And since direct liraglutide-specific measurements of skeletal muscle glycogen in humans are still missing, the most accurate way to describe glycogen repletion is mechanistically plausible rather than proven.
Translational Limits for U.S. Clinical Use
This is where lab data meets clinic reality. What matters most is whether these signals show up in human outcomes, and right now the human evidence is still indirect because studies rarely measure skeletal muscle GLUT4 or glycogen directly.
For U.S. clinicians, the safest framing is straightforward: liraglutide’s effects on muscle GLUT4 may help explain part of its glycemic benefit, but they are not a validated muscle-glycogen endpoint. Strong animal data can point us in a direction, but they don’t prove better human muscle glycogen storage or better performance. That distinction matters in patient counseling, especially when mechanistic findings are still being tested in humans.
Clinical Takeaways for Peptide Practice
Most of the data here comes from preclinical work, and the long-term findings are mixed. So the practical job for clinicians is pretty simple: use the data carefully, and don't stretch it beyond what it shows.
What Clinicians Can Reasonably Take From the Evidence
The clearest point from the literature is this: in acute preclinical models, liraglutide increased cAMP, activated AMPK, phosphorylated AS160/TBC1D1, and promoted GLUT4 translocation in skeletal muscle cells.
But that doesn't mean the whole story is settled. Chronic effects in healthy muscle have been less consistent, with no significant increase in membrane GLUT4 or glucose uptake.
That split matters. Normal muscle and insulin-resistant muscle may not react the same way. The clearest signal comes from insulin-resistant models, where liraglutide improved skeletal muscle insulin signaling. In animals with normal glucose tolerance, that effect was not seen. So the glycogen idea is reasonable to discuss, but it still hasn't been proven in humans.
How to Present This Mechanistic Data in Practice
When talking with patients, keep the message tight. Present the GLUT4 data as mechanistic context, not as a reason to prescribe. In plain terms, it may help explain improved glucose disposal, but it does not prove a direct muscle-glycogen effect.
It's also smart to document that distinction clearly. If muscle-metabolism mechanisms come up in a patient conversation, note in the chart that you separated approved indications from mechanistic ideas drawn from preclinical models. That helps keep expectations grounded and protects both the patient and the clinician.
Using PeptidePrescriber to Organize the Evidence
For clinicians who want to keep this material organized, structured references can help separate mechanism-focused data from approved-use claims. PeptidePrescriber gives licensed prescribers evidence-based monographs, dosing protocols, calculators, injection guides, and regulatory references to organize liraglutide use within approved indications.
Conclusion: What the Current Evidence Supports
Preclinical data support a plausible liraglutide-GLUT4 mechanism in skeletal muscle, especially in insulin-resistant models. Across these studies, the signal points in the same direction. Even so, the human clinical story still rests on systemic outcomes, not direct evidence from muscle tissue.
That’s the main gap. We still don’t have direct human skeletal muscle data under clinical dosing conditions. There’s also a mismatch between the concentrations and models used in cell and rodent work and what patients are exposed to at standard clinical doses. So while the preclinical case is strong enough to support the idea, it can’t settle the question by itself.
For clinicians, the practical takeaway is pretty straightforward: liraglutide’s muscle GLUT4 effect is hypothesis-supporting, not decision-driving. The best human evidence remains systemic rather than muscle-specific.
Bottom Line for U.S. Clinicians
Liraglutide likely helps improve muscle glucose handling in insulin-resistant states through AMPK- and Akt-linked pathways. In practice, focus on HbA1c, weight, and insulin sensitivity as the main clinical endpoints. Treat GLUT4 as useful mechanistic context, not as a reason to prescribe on its own.
FAQs
Does liraglutide increase GLUT4 in human muscle?
The search results provided here do not show whether liraglutide increases GLUT4 in human muscle.
For licensed healthcare professionals, PeptidePrescriber offers evidence-based peptide therapy resources, including monographs, dosing protocols, and regulatory references.
Is the effect stronger in insulin-resistant muscle?
Current evidence does not directly show whether liraglutide has a stronger effect on GLUT4 translocation in insulin-resistant muscle than in healthy muscle.
What the literature does show is that GLP-1 receptor agonists can improve insulin resistance and overall glycemic control. But it stops short of making that specific head-to-head mechanistic comparison.
Can liraglutide improve muscle glycogen repletion?
Liraglutide may indirectly help muscles take up glucose and refill glycogen stores by improving insulin sensitivity and blood sugar control.
It mainly works by increasing glucose-dependent insulin secretion and lowering glucagon. But those effects can also create a better setting for skeletal muscle to use glucose more efficiently.