Here’s the short answer: GLP-1 drugs lower blood sugar mostly by helping the body make insulin when glucose is high, lowering glucagon, and slowing how fast food leaves the stomach. They do improve insulin-driven glucose uptake in some people, but that effect shows up most clearly in obesity, insulin resistance, and type 2 diabetes.
If you want the plain-English version, it’s this:
- The strongest human data are for post-meal glucose control
- Clamp studies show better whole-body glucose disposal when insulin is already high
- Direct muscle and fat uptake effects in humans are still not well proven
- Short-acting GLP-1 drugs help more with meal spikes
- Long-acting drugs help more with all-day glucose control (see our practical clinical guides for administration details)
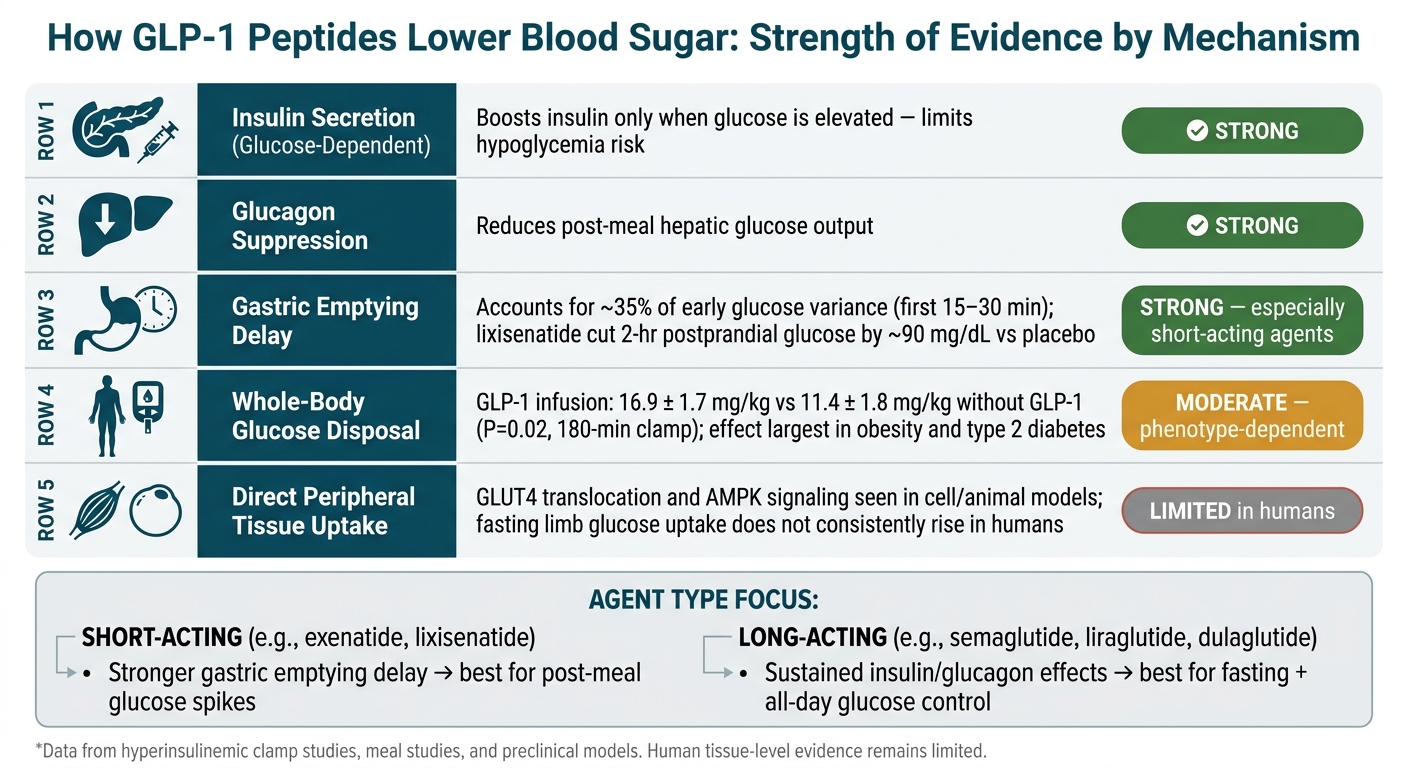
A few numbers make that clearer. In one clamp study in older adults, GLP-1 increased whole-body glucose uptake from 11.4 ± 1.8 mg/kg to 16.9 ± 1.7 mg/kg over 180 minutes. In meal studies, lixisenatide cut 2-hour postprandial glucose by about 90 mg/dL versus placebo. And delayed gastric emptying explains about 35% of early glucose changes in the first 15 to 30 minutes after oral carbohydrate.
My take: most of the glucose-lowering effect comes from upstream hormone and gut effects, not from a clear, steady push of glucose straight into muscle or fat. The tissue-level story is still more certain in lab and animal work than in people.
GLP-1 Peptides: Mechanisms of Glucose Lowering at a Glance
GLP-1 Receptor Agonists | Incretin Therapies for Type 2 Diabetes | Management of Diabetes Mellitus
sbb-itb-7164bd9
Quick Comparison
| Area | What the data show | Best fit |
|---|---|---|
| Insulin secretion | GLP-1 boosts insulin only when glucose is high | Strong human support |
| Glucagon suppression | Lowers liver glucose output after meals | Strong human support |
| Gastric emptying | Slows glucose entry into the bloodstream | Strong human support, strongest with short-acting agents |
| Whole-body glucose uptake | Improves during hyperinsulinemic clamp settings | Seen most in insulin-resistant groups |
| Direct muscle/fat uptake | Seen in preclinical models more than in human studies | Human proof is limited |
So if you’re asking, “Do GLP-1 peptides increase insulin-mediated glucose uptake?” my answer is: yes, but mostly under insulin-stimulated conditions, and not as the main reason these drugs lower glucose. The main clinical effect still comes from better post-meal control, lower glucagon, and slower glucose entry.
Human Studies on Insulin Sensitivity and Whole-Body Glucose Uptake
Human clamp studies point to a pretty consistent pattern: GLP-1 pathway peptides help the body dispose of more glucose when insulin is already up. The big issue isn’t whether they affect glucose handling at all. It’s when that effect shows up - during controlled insulin stimulation or during basal conditions.
Clamp and Infusion Study Findings
The main takeaway from clamp studies is straightforward. GLP-1 receptor agonism improves whole-body insulin-stimulated glucose disposal mainly under hyperinsulinemic conditions. In these studies, exenatide and liraglutide increased insulin-stimulated glucose disposal and glucose infusion rates. That means GLP-1 receptor agonism most clearly improves whole-body uptake when insulin levels are elevated. In other words, it seems to boost insulin-stimulated uptake rather than drive insulin-independent uptake on its own.
A mechanistic clamp study comparing cotadutide with liraglutide found a similar pattern. Both agents significantly increased glucose disposal and suppressed hepatic glucose output during clamps.
One of the more striking data points comes from GLP-1 infusion in older adults during a nutrient-stimulated clamp. Over 180 minutes, whole-body glucose uptake was 16.9 ± 1.7 mg/kg with GLP-1 versus 11.4 ± 1.8 mg/kg without it (P = 0.02). GLP-1 also increased skeletal muscle microvascular perfusion and was linked to higher glucose uptake under nutrient-stimulated conditions. Skeletal muscle microvascular blood flow increased by roughly 5-fold with GLP-1, compared with a 2-fold increase from feeding alone (P = 0.008). That suggests part of the glucose-disposal effect may come from better vascular delivery to muscle tissue.
There’s an interesting contrast in acute infusion studies in healthy volunteers. GLP-1 infusion at physiologic concentrations increases skeletal and cardiac muscle microvascular perfusion, but it does not significantly increase muscle glucose uptake in the fasted, euglycemic state. So blood flow can go up without a matching rise in glucose flux. That split matters. It supports the idea that GLP-1’s tissue-level effects on glucose uptake are still driven mostly by the presence of insulin.
Responses by Patient Population
The size of the response also depends on who you’re looking at. People with more baseline insulin resistance have more room to improve, so the effect tends to be larger in patients with type 2 diabetes or obesity.
In elderly patients with type 2 diabetes, 12 weeks of continuous subcutaneous GLP-1 infusion increased clamp-measured glucose disposal and reduced hepatic glucose output. That points to insulin-sensitizing effects that persist over a 12-week period.
In healthier adults, the effect is still there, but it’s smaller. Short-term liraglutide can increase clamp glucose infusion rates, though the absolute change is more modest because baseline insulin sensitivity is already fairly high.
The tirzepatide-versus-semaglutide comparison adds another piece to the puzzle. Clamp data show that tirzepatide produced a greater improvement in insulin sensitivity relative to weight loss than semaglutide. That hints at effects that go beyond weight loss alone and helps explain why meal-related glucose control can improve even when fasting glucose uptake changes very little.
Postprandial Glucose Control, Insulin Secretion, and Gastric Emptying
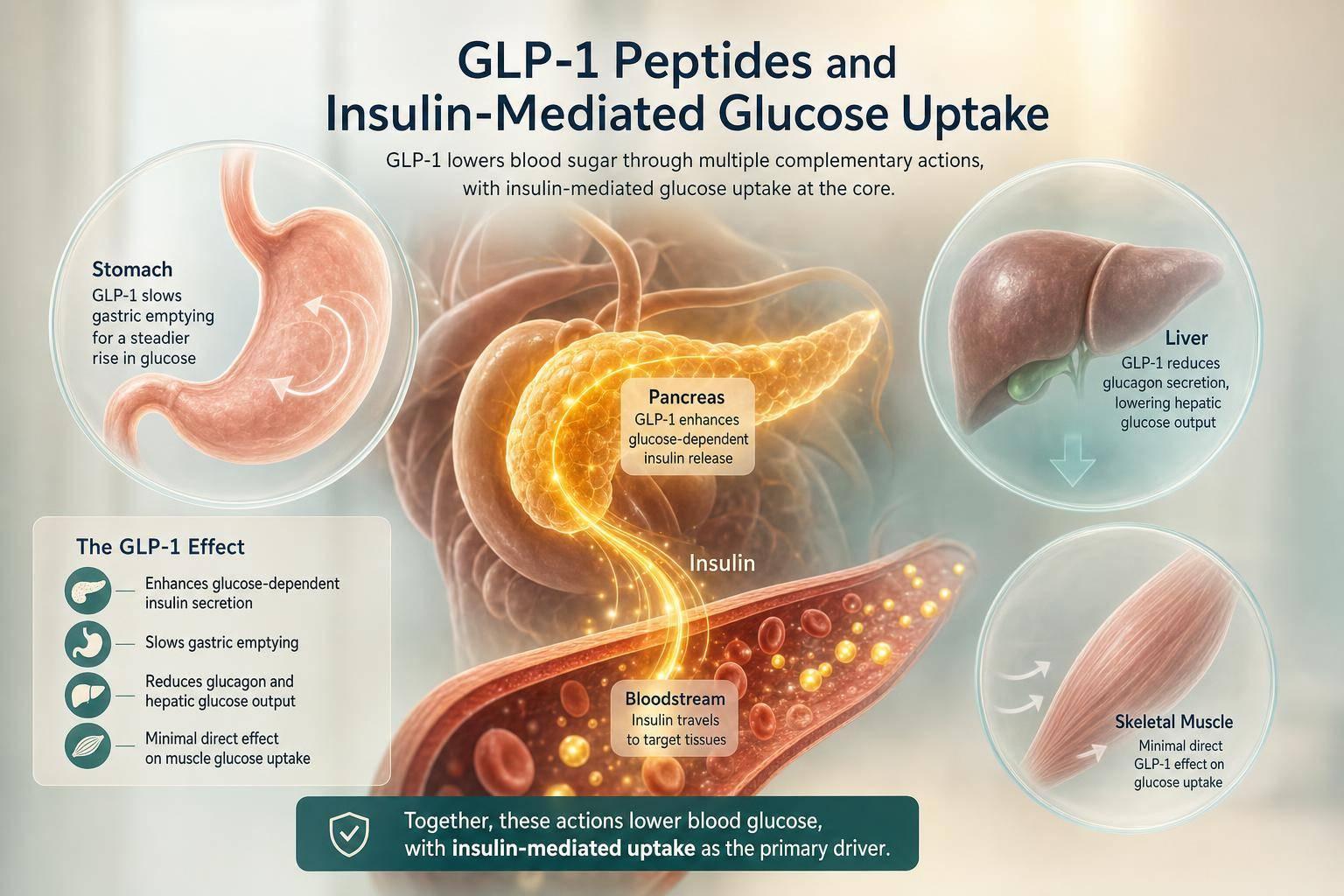
Clamp studies show better insulin-stimulated glucose disposal. Meal studies help show why that leads to lower postprandial glucose. After eating, GLP-1 pathway peptides lower glucose in three main ways: they increase insulin only when glucose goes up, suppress glucagon, and slow nutrient delivery. That matters because these changes affect how much glucose reaches the bloodstream before peripheral tissues have to clear it. Put simply, GLP-1 works upstream of peripheral glucose disposal, which is why meal-time glucose often improves more than fasting uptake alone would suggest.
Insulin and Glucagon Changes After Meals
GLP-1 stimulates insulin only when glucose is elevated, which limits hypoglycemia.
In people with type 2 diabetes, acute GLP-1 infusion and short-acting agents such as exenatide can improve first-phase insulin response during meals. In practice, that means lower post-meal glucose peaks for equal or only slightly higher insulin levels.
Glucagon suppression is another major part of the story. In T2D, post-meal glucagon is often inappropriately elevated. GLP-1 receptor signaling suppresses post-meal glucagon, which lowers hepatic glucose output and helps flatten the later rise in postprandial glucose.
Gastric Emptying and Rate of Glucose Entry Into Circulation
Beyond the pancreatic islets, gastric emptying has a big effect on the early glucose rise. Delayed gastric emptying accounts for about 35% of the variance in plasma glucose during the first 15 to 30 minutes after an oral carbohydrate load in both healthy people and people with diabetes. By slowing nutrient delivery to the small intestine, GLP-1 pathway peptides reduce the rate of glucose entry into circulation and blunt the early post-meal peak.
In healthy volunteers, acute GLP-1 can reduce measured post-meal insulin secretion because less glucose reaches the bloodstream early.
Short-acting agents such as twice-daily exenatide and lixisenatide cause a stronger delay in gastric emptying around the time of dosing, which makes them especially useful for blunting postprandial spikes. Lixisenatide, for example, reduced 2-hour postprandial glucose by about 90 mg/dL versus placebo in phase II/III data.
Long-acting agents such as liraglutide, semaglutide, and dulaglutide still slow gastric emptying, but that effect tends to lessen with continuous exposure. In one randomized study, once-weekly semaglutide showed a first-hour gastric emptying AUC ratio of 0.73 (95% CI 0.61–0.87) versus placebo, while overall emptying across the full postprandial period was similar to placebo. So their effect after meals depends more on insulin and glucagon changes than on gastric slowing.
A simple way to think about agent choice:
- Short-acting agents fit patients with dominant post-meal spikes.
- Long-acting agents fit cases where both fasting and postprandial control need work.
That upstream control of glucose entry helps frame the next question: what preclinical data show about tissue-level glucose handling in skeletal muscle and adipose tissue.
Preclinical and Translational Data on Peripheral Tissue Glucose Handling
Preclinical and translational work suggests that GLP-1 signaling may also act directly on skeletal muscle and adipose tissue glucose handling. That said, the effect looks smaller and less steady than its actions in the islets and the stomach. In people, the evidence is still mostly indirect. The clearest direct uptake effects show up in cell and animal studies. So the key issue is simple: do these gains go beyond hormone and gut effects and reach the tissues that clear glucose?
Skeletal Muscle Glucose Transport and Signaling
Skeletal muscle is the clearest place to test that idea. It handles most insulin-mediated glucose uptake, so even modest shifts can matter.
In human muscle strips, myotubes, and satellite cells, GLP-1 increased glycogen synthesis and glucose uptake through PI3K-linked and AMPK/TBC1D1-dependent pathways. GLUT4 translocation has also been reported in rodent and cell models. Rodent studies point in the same direction, showing better muscle glucose uptake and insulin sensitivity, with AMPK signaling tied to the effect.
In humans, GLP-1 infusion increases skeletal muscle microvascular recruitment, but fasting limb glucose uptake often does not go up when GLP-1 is infused on its own. Put another way, better blood flow may help set the stage, but it doesn't appear to be enough by itself to drive more glucose uptake.
There’s another twist here. In human myocytes, the gain showed up mainly in cells derived from people with obesity, not in samples from healthy people or those with type 2 diabetes.
Adipose Tissue Glucose Handling
The adipose tissue story is murkier. These signals are weaker, and it’s harder to separate direct tissue effects from the impact of weight loss. In vitro, GLP-1 agonists increase glucose uptake and GLUT4 trafficking. In humans with obesity, treatment can improve adipocyte insulin sensitivity and antilipolytic responses. At the same time, weight loss, lower ectopic fat, and reduced free fatty acids likely play a part too.
Taken together, the case is strongest for direct effects in skeletal muscle. For adipose tissue, the data are weaker and more tangled up with changes in body weight and fat distribution. These peripheral effects also seem most visible in metabolically unhealthy tissue, which may help explain why clinical glucose lowering can be greater than fasting clamp data alone would suggest.
Integrated Interpretation and Clinical Takeaways
What the Current Evidence Supports
Taken together, the human studies point first to upstream control of glucose entry and islet signaling, not to a uniform direct increase in tissue uptake. In plain terms, GLP-1 peptides seem to lower glucose mainly by changing how glucose gets into the system and how the pancreas responds, rather than by consistently pushing more glucose into muscle or fat.
There’s a clear pecking order in the data. The strongest support is for postprandial glucose control. The support for insulin-mediated whole-body glucose disposal is more modest and depends on the patient group. And the support for direct peripheral tissue uptake in humans is the weakest.
Postprandial glucose control is where the evidence is strongest. Both subcutaneous and oral semaglutide lower early postprandial glucose and slow early gastric emptying, while total 5-hour emptying stays largely unchanged. That same pattern shows up across formulations.
Effects on insulin-mediated whole-body glucose disposal are modest and phenotype-dependent. Clamp studies show better insulin sensitivity, with larger effects in obesity and type 2 diabetes than in lean or insulin-replete phenotypes.
Clamp studies also come with an important limit: they measure whole-body disposal, not tissue-specific flux. So while preclinical work can help explain how these drugs may act, it does not prove what happens in human muscle or fat. Direct muscle and fat effects remain plausible but unproven in humans. Preclinical findings suggest these tissue effects may exist, but human confirmation is still limited. It makes sense to treat those findings as mechanistic clues, not clinical proof.
Key Points for Prescriber Interpretation
For prescribers, the near-term story is fairly straightforward. Early post-meal improvement appears to come from slowed gastric emptying, glucose-dependent insulin secretion, and glucagon suppression. Over time, changes in fasting glucose and insulin needs seem more tied to shifts in insulin sensitivity and glucagon tone.
Population matters here. Lean, insulin-replete phenotypes show less clear benefit for glucose uptake than insulin-resistant phenotypes.
Conclusion: What GLP-1 Peptide Data Show
GLP-1 peptides reliably blunt postprandial glucose, improve insulin-mediated disposal mainly in insulin-resistant phenotypes, and show only limited human evidence for direct peripheral uptake effects.
FAQs
Do GLP-1 drugs directly increase muscle glucose uptake?
No. GLP-1 receptor agonists do not directly increase glucose uptake in skeletal muscle.
Instead, they improve glucose handling indirectly. They do this by stimulating glucose-dependent insulin secretion, suppressing glucagon, slowing gastric emptying, and improving insulin sensitivity.
Better glycemic control and weight loss can also help support more normal glucose handling in tissues.
Why do GLP-1 drugs help more with post-meal glucose than fasting glucose?
GLP-1 receptor agonists mainly help with post-meal glucose.
Here’s why: they trigger insulin release only when blood glucose is high, which usually happens after eating. That means they work when the body needs extra help, instead of pushing insulin all the time.
They also slow gastric emptying. In plain English, food leaves the stomach more slowly, so glucose enters the bloodstream at a slower pace. Put those two effects together, and you get better control over postprandial spikes with a lower risk of hypoglycemia during fasting.
Who benefits most from GLP-1 effects on insulin sensitivity?
People with type 2 diabetes, obesity, or metabolic syndrome are often the ones most likely to benefit from GLP-1 effects on insulin sensitivity.
These treatments are meant in particular for people with a BMI of 30 kg/m² or higher, or 27 kg/m² or higher if they also have weight-related conditions such as hypertension or dyslipidemia. In plain terms, they can help the body respond better to insulin, handle glucose more effectively, and improve overall glycemic control.