
Managing side effects during peptide therapy, especially gastrointestinal (GI) issues, is all about starting low, increasing doses slowly, and making small lifestyle adjustments. Here's what you need to know:
- Common GI Symptoms: Nausea (15–80%), diarrhea (8–30%), and constipation (5–35%) are frequent with GLP-1 agonists like semaglutide and tirzepatide. These often occur in the first week or after dose increases.
- Key Strategies: Start with the lowest dose (e.g., 0.25 mg weekly for semaglutide), increase gradually every 4–8 weeks, and adjust based on patient tolerance and selection criteria.
- Diet Tips: Opt for smaller meals, avoid high-fat or spicy foods, stay hydrated, and avoid lying down after eating.
- When to Pause or Stop: Severe symptoms like intense nausea, vomiting, or abdominal pain may require dose adjustments, temporary pauses, or stopping therapy altogether.
Peptide therapy can be effective, but managing side effects requires careful planning and clear communication with patients. Proper dosing and preparation make a big difference in improving treatment success.
Managing the Gastrointestinal Side Effects of GLP-1s: Focus on Nutrition & Lifestyle Interventions
sbb-itb-7164bd9
Baseline Assessment and Patient Preparation
A thorough pre-therapy evaluation is key to reducing severe gastrointestinal (GI) side effects. This step is a vital part of the dosing checklist for peptide therapy, ensuring patients are well-prepared and potential risks are minimized.
Conducting a GI Risk Assessment
Start by reviewing the patient's medical history. It's crucial to rule out absolute contraindications, such as a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), before prescribing GLP-1 agonists. Be on the lookout for conditions like pancreatitis, severe gastroparesis, gallbladder disease, or inflammatory bowel disease, as these can increase GI-related risks.
Examine current medications carefully. Since GLP-1 agonists slow gastric emptying, they can impact the absorption of drugs with narrow therapeutic windows.
"GLP-1 agonists slow gastric emptying, which can alter the absorption of orally administered drugs. This matters for medications with narrow therapeutic windows like oral contraceptives, warfarin, levothyroxine, and certain antibiotics." - Peptide Association
Baseline lab work is non-negotiable. The table below highlights key tests to conduct before starting therapy:
| Lab Test | Purpose |
|---|---|
| Lipase & Amylase | Establish a baseline for pancreatic health and monitor pancreatitis risk |
| Thyroid Panel (incl. Calcitonin) | Screen for potential risks of medullary thyroid carcinoma |
| CMP (Renal/Hepatic) | Evaluate hydration status and drug clearance ability |
| HbA1c / Fasting Glucose | Assess hypoglycemia risk when combined with other medications |
Additionally, document any pre-existing GI symptoms, such as nausea, bloating, or irregular bowel movements. This helps differentiate between issues caused by therapy and those that were present beforehand.
Dietary and Behavioral Counseling
Proper dietary preparation can ease early GI symptoms. Since slowed gastric emptying makes heavy meals harder to handle, suggest smaller, more frequent meals and stress the importance of stopping when feeling full. Advise patients to limit high-fat, greasy, or spicy foods during the titration phase.
Encourage patients to stay upright for 30–60 minutes after eating to aid digestion and reduce reflux. They should also sip fluids consistently throughout the day to maintain hydration without overloading their stomachs.
Setting Patient Expectations
Clear communication about potential side effects is crucial. Nausea is reported by 20% to 44% of semaglutide users, while diarrhea, vomiting, and constipation occur in approximately 24% to 30% of patients during titration. These symptoms are usually temporary, peaking during the first few weeks or after a dose increase, and often subside within 4 to 8 weeks as the body adjusts.
Teach patients to recognize serious symptoms. They should contact the clinic immediately if they experience severe abdominal pain radiating to the back (a possible sign of pancreatitis), intractable vomiting, or bloody stools. By distinguishing between common, mild side effects and more serious warning signs, patients can feel more confident in managing their treatment journey safely.
Dosing and Titration Strategies to Reduce GI Events
Peptide Therapy Dosing: GI Side Effect Management Protocol
Starting with the right dose is key to minimizing gastrointestinal (GI) side effects. The aim is not to rush to the maintenance dose but to achieve it gradually and comfortably.
Selecting a Starting Dose
It's best to begin with the lowest effective dose. For example, start with 0.25 mg weekly for semaglutide or 2.5 mg for tirzepatide. These doses aren't meant to be therapeutic but to help the GI tract adjust to slowed gastric emptying before full receptor engagement occurs.
In the STEP 1 trial, 44.2% of participants taking semaglutide 2.4 mg experienced nausea, compared to 17.4% in the placebo group.
Before starting, confirm baseline lab values to ensure safe titration. Once a starting dose is determined, increasing it gradually helps reduce the likelihood of GI discomfort.
Gradual Dose Escalation
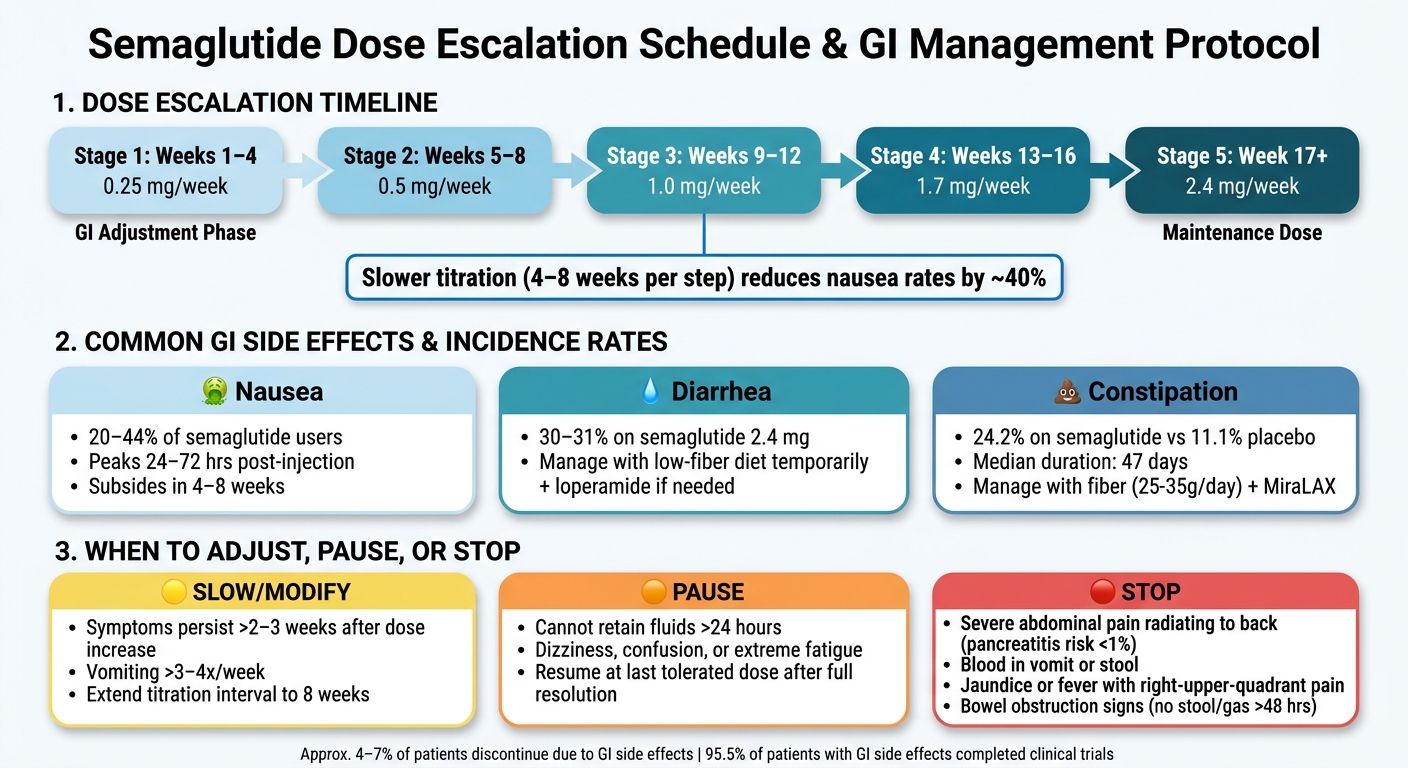
A widely used approach is to maintain each dose for about four weeks before moving to the next level. This allows the GI system to adapt, and studies show that slower titration can lower nausea rates by approximately 40% compared to faster escalation.
| Treatment Period | Semaglutide (Wegovy) Weekly Dose |
|---|---|
| Weeks 1–4 | 0.25 mg |
| Weeks 5–8 | 0.5 mg |
| Weeks 9–12 | 1.0 mg |
| Weeks 13–16 | 1.7 mg |
| Week 17 onward | 2.4 mg (Maintenance) |
If patients experience significant GI symptoms, they can remain on their current dose for an additional four weeks. With careful titration, the rate of discontinuation due to GI issues typically stays below 5%.
"Dose escalation protocols are not administrative procedures. They are a biological necessity." - BioStrata Research Editorial Team
Injection Timing and Technique
After titration, proper injection timing and technique can further reduce GI events. Administering the injection in the evening with a meal containing moderate fat may lessen GI symptoms. Alternatively, some protocols suggest morning injections so that any nausea occurs during waking hours.
For better comfort, let refrigerated medication sit at room temperature for 10–15 minutes before injecting to avoid stinging and irritation. Rotate injection sites - abdomen, thigh, or upper arm - and avoid using the same area more than once in two weeks. Injecting slowly can also help minimize irritation.
For prescribers looking to create educational materials, PeptidePrescriber provides a clinical injection site guide and a library of dosing protocols to support consistent, evidence-based practices.
Managing Common GI Symptoms
Even with careful dose adjustments, some patients may still deal with gastrointestinal (GI) symptoms. Thankfully, most cases are mild to moderate and can be addressed with specific strategies.
Managing Nausea
Nausea is the most frequently reported GI issue in peptide therapy, affecting 20% to 44% of patients. It usually peaks within 24–72 hours after an injection or dose increase and tends to subside after 4–8 weeks once a stable dose is established.
To ease nausea, try eating smaller meals, avoiding greasy or high-fat foods, eating slowly, and stopping as soon as you feel full. Staying hydrated is equally important - sip fluids steadily without overloading your stomach. Natural remedies like ginger, peppermint tea, or acupressure wristbands can also help. If medication is necessary, prochlorperazine is often preferred over ondansetron, as ondansetron can worsen constipation, a common side effect of GLP-1 peptide therapy.
Using the CTCAE grading scale can guide dosing adjustments. For instance, Grade 2 nausea, which involves reduced oral intake, signals the need to pause dose increases until symptoms improve to Grade 1.
"The fastest way to manage GLP-1 nausea is usually to shrink meal size, keep food lower in fat, eat more slowly, sip fluids steadily, and avoid increasing the dose if the current one is still making it hard to eat or drink." - Krishna Patel, MD
For those experiencing vomiting or diarrhea, similar dietary and dosing adjustments can be applied.
Managing Diarrhea and Vomiting
Vomiting occurs in approximately 25% of patients taking semaglutide 2.4 mg and 10–12% of those on tirzepatide 15 mg. Diarrhea is also common, with semaglutide 2.4 mg clinical trials reporting rates of 30–31%.
Vomiting generally indicates intolerance. If it happens, step back to the last well-tolerated dose instead of stopping the therapy altogether.
"Vomiting parallels severe hypoglycaemia, indicating intolerance significant enough to stepping back to the last well tolerated level." - Abdulhameed Alhazmi, Internal Medicine, Jazan University Hospital
To manage diarrhea, consider temporarily reducing high-fiber foods and dairy while your body adjusts. Avoid coffee, alcohol, carbonated drinks, and foods containing sugar alcohols like sorbitol or xylitol, as these can worsen symptoms. If dietary changes don't resolve the issue, a short-term course of loperamide may help. Staying hydrated with small, frequent sips is crucial to prevent dehydration and reduce the risk of kidney problems.
Seek medical attention if vomiting occurs more than 3–4 times a week or if severe abdominal pain radiates to the back, as these could indicate more serious complications.
Managing Constipation
Constipation affects about 24.2% of patients on semaglutide 2.4 mg compared to 11.1% on placebo, with episodes lasting a median of 47 days. This side effect is primarily due to slowed colonic motility, which is part of the drug's mechanism of action.
To manage constipation, increase water intake to 73–100 oz daily, aim for 25–35 g of fiber per day, and include 20–30 minutes of physical activity in your routine to encourage bowel movements. Psyllium husk is a practical fiber option - start with 1 teaspoon (5 g) in 8 oz of water daily and gradually increase to 3 teaspoons (15 g) spread across meals.
For additional support, Polyethylene Glycol 3350 (MiraLAX) is a common first-line laxative. Magnesium oxide (400 mg) or magnesium citrate (200–400 mg) at bedtime are also effective alternatives. Stimulant laxatives like bisacodyl or senna should only be used occasionally, as regular use may lead to dependency. Docusate sodium (Colace) is less effective and often performs similarly to a placebo.
Constipation risk peaks 1–3 days after an injection when drug levels are highest, so focus on hydration and fiber during this time. If constipation is accompanied by severe symptoms like persistent vomiting, abdominal pain, bloating, or inability to pass gas, seek immediate medical care.
When to Adjust, Pause, or Stop Therapy
Adjusting therapy based on a patient's response is crucial, especially when managing gastrointestinal (GI) symptoms. The timing and nature of these adjustments can significantly impact treatment outcomes. If initial strategies to manage symptoms aren't effective, it's essential to modify the approach.
When to Slow or Modify Doses
If GI symptoms persist for more than 2–3 weeks after increasing the dose, it's better to hold the current dose rather than escalate it further. For cases where vomiting occurs more than 3–4 times a week or nausea doesn't improve after 2 weeks at the same dose, consider lowering the dose.
Patients with heightened GI sensitivity may benefit from a slower titration process. Extending the interval between dose increases from the usual 4 weeks to 8 weeks can give their bodies more time to adjust. Similarly, those with specific conditions - like a history of abdominal surgery, ongoing opioid use, or pre-existing gastroparesis - require more cautious dose adjustments and closer monitoring.
When to Temporarily Pause Therapy
In certain situations, a temporary pause in therapy is necessary to ensure patient safety. For instance, if a patient cannot retain fluids for over 24 hours, therapy should be paused immediately to prevent dehydration and potential kidney issues.
Other red flags include dizziness, confusion, or extreme fatigue occurring alongside vomiting, as these symptoms may indicate volume depletion. Once symptoms have fully resolved, treatment can resume at the last dose that was well-tolerated. It's recommended to maintain this dose for 2–4 additional weeks before considering any further increases.
"Withhold treatment temporarily until the resolution of AEs and then resume treatment." - MDPI Expert Consensus
If symptoms worsen even after pausing therapy, further intervention may be necessary.
When to Permanently Stop Therapy
In some cases, stopping therapy altogether becomes unavoidable. If GI symptoms persist despite dose adjustments and pose a continued risk to the patient's safety, discontinuation should be considered. According to clinical data, about 4–7% of patients ultimately stop therapy due to GI side effects.
Immediate discontinuation is required if any of the following occurs:
- Severe abdominal pain radiating to the back – this could indicate acute pancreatitis, a rare but serious condition affecting less than 1% of patients.
- Inability to pass stool or gas for over 48 hours, especially if accompanied by abdominal distension, suggesting a possible bowel obstruction.
- Vomiting blood or finding blood in stools.
- Jaundice or fever with chills and right-upper-quadrant pain, which may signal gallbladder issues like cholecystitis or gallstones.
- Intense and persistent GI symptoms that don't improve despite dose reductions or other interventions.
It's helpful to establish clear criteria for discontinuation before starting therapy. This proactive approach ensures both patients and healthcare providers are prepared to make timely decisions.
For detailed peptide dosing protocols and additional resources, healthcare professionals can visit PeptidePrescriber.
Conclusion: Key Steps for Reducing GI Side Effects
Effectively managing GI side effects during peptide therapy calls for a steady and methodical approach, with gradual dose increases being the cornerstone. Studies show that extending the dose escalation period to 4–8 weeks can cut nausea and other GI symptoms by 30–40% compared to more aggressive schedules. Since about 80% of GLP-1 users encounter GI issues within the first week of treatment, starting with the lowest possible dose and increasing it slowly is key to easing these symptoms.
It's also helpful to inform patients that GI symptoms tend to peak during dose adjustments but usually subside within 2–3 weeks. Sharing data like this can boost adherence - especially since pooled clinical trials reveal that 95.5% of participants who experienced GI side effects were still able to complete their studies. This statistic can provide reassurance and encourage patients to stick with their treatment plan.
In addition to careful dosing, patient education tips can make a big difference. Evening injections, eating moderate-fat meals on injection days, and staying well-hydrated (around 68–101 fluid ounces daily) are practical strategies that can help reduce the severity of symptoms. These small adjustments can go a long way in improving the overall experience for patients.
FAQs
How do I know if my GI symptoms are normal or dangerous?
Mild nausea, occasional reflux, or shifts in bowel habits often occur as peptides slow down gastric emptying. These effects typically peak after increasing your dose and tend to improve with time.
However, if you experience severe abdominal pain (especially if it spreads to your back), ongoing vomiting, dehydration, or symptoms that persist or worsen for more than two weeks after a dose adjustment, seek medical attention immediately.
What should I do if I miss a dose during titration?
When it comes to missed doses during titration, specific guidance isn't outlined in the article. It's always best to consult your prescribing healthcare provider for advice tailored to your specific medication and dosing schedule. For clinicians seeking evidence-based resources and protocols, PeptidePrescriber provides professional tools designed to support the safe and effective management of peptide therapy.
Can GLP-1 peptides affect how my other oral medications work?
GLP-1 peptides can influence the way oral medications work by slowing down gastric emptying. This means it might take longer for these medications to reach their peak levels in your bloodstream, and those peak levels could be slightly reduced. However, the total amount of the medication absorbed generally remains the same.
Special care is needed for medications with a narrow therapeutic index, such as oral contraceptives or levothyroxine, as their effectiveness could be affected. Additionally, if you're taking insulin or sulfonylureas, dosage adjustments might be necessary to reduce the risk of hypoglycemia.