Peptides are small chains of amino acids that play a central role in controlling hunger and fullness by acting as messengers between the gut, bloodstream, and brain. They regulate appetite through two types of signals: orexigenic (hunger-promoting) and anorexigenic (appetite-suppressing). These signals work together to manage food intake and energy balance.
Key points:
- Short-term regulation: Peptides like ghrelin (triggers hunger) and GLP-1, PYY, and CCK (promote fullness) manage meal size and frequency.
- Long-term regulation: Hormones like leptin (from fat cells) and insulin (from the pancreas) help maintain energy reserves by acting on the brain.
- Disruptions, such as leptin resistance in obesity, make weight management harder by weakening fullness signals.
- Treatments like semaglutide and tirzepatide target these pathways, helping patients lose 15–22% of body weight by enhancing satiety and reducing hunger.
Peptide-based therapies offer a way to address both physiological hunger and food cravings, making them effective tools in weight management.
PYY is a Satiety Hormone | Part 7 Neurobiology of Food Intake | Macronutrients Lecture 43
sbb-itb-7164bd9
How Appetite and Satiety Are Regulated
Appetite regulation is a complex process involving constant communication between the gut, bloodstream, and brain. This intricate system determines when you feel hungry, how much you eat, and when you feel full. It’s a balancing act that connects the immediate signals from meals with the body’s long-term energy needs.
The Gut–Brain Axis: The Gut’s Communication Network
The gut is more than just a digestive organ - it’s a key player in sensing and signaling. Enteroendocrine cells (EECs), which make up less than 1% of the gut’s epithelial cells, are crucial here. Despite their small numbers, they form the largest endocrine system in the body. These cells detect nutrients using specialized receptors called GPCRs.
When food enters the gut, these cells release peptides like GLP-1, PYY, and CCK. These peptides communicate with the brain through two main routes:
- Neural Pathway: Signals travel along vagal afferent neurons, which are densely connected to the gut. These neurons relay information about gut stretch and nutrient composition directly to the brainstem’s Nucleus of the Solitary Tract (NTS).
- Humoral Pathway: Peptides enter the bloodstream and reach the brain via circumventricular organs, such as the Area Postrema, which lack a complete blood-brain barrier.
"The gut–brain axis is a bidirectional communication pathway connecting the gut and brain, using hormonal and neural signals to regulate metabolic homeostasis." – Nutrients
These pathways meet at the Arcuate Nucleus (ARC) in the hypothalamus, the brain’s central hub for appetite control. The ARC houses two key neuron groups: NPY/AgRP neurons, which stimulate hunger, and POMC/CART neurons, which signal fullness.
The timing of these signals is essential - it determines whether they provide short-term satiety after a meal or contribute to long-term energy balance.
Short-Term vs. Long-Term Appetite Regulation
Appetite regulation operates on two distinct timelines: short-term and long-term.
- Short-Term Signals: These respond to what’s happening in your gut during meals. Peptides like GLP-1, PYY, and CCK are released as you eat, promoting feelings of fullness. Meanwhile, ghrelin levels rise before meals to trigger hunger. These signals primarily travel via the vagus nerve to the brainstem, influencing how much you eat and how often, on a timescale of minutes to hours.
- Long-Term Signals: These focus on maintaining your body’s energy reserves over days, weeks, or even months. Hormones like leptin (produced by fat cells) and insulin (produced by the pancreas) circulate in the bloodstream in amounts proportional to body fat. They act directly on the hypothalamus to ensure energy stores remain balanced.
Here’s a quick comparison of these two systems:
| Feature | Short-Term Signals | Long-Term Signals |
|---|---|---|
| Primary goal | Manage meal size and frequency | Regulate body fat and energy storage |
| Key peptides | Ghrelin, CCK, PYY, GLP-1 | Leptin, Insulin |
| Primary source | Gastrointestinal tract | Fat tissue and pancreas |
| Main pathway | Vagus nerve → brainstem (NTS) | Bloodstream → hypothalamus (ARC) |
| Timescale | Minutes to hours | Days to months |
These systems don’t work in isolation. For example, in obesity, long-term signaling often breaks down. A condition called leptin resistance occurs when the brain stops responding to leptin’s satiety signals, even when leptin levels are high. This disruption makes weight management far more challenging than simply eating less, requiring careful patient selection criteria for peptide therapy to ensure effective treatment.
Key Peptides and Hormones That Influence Appetite
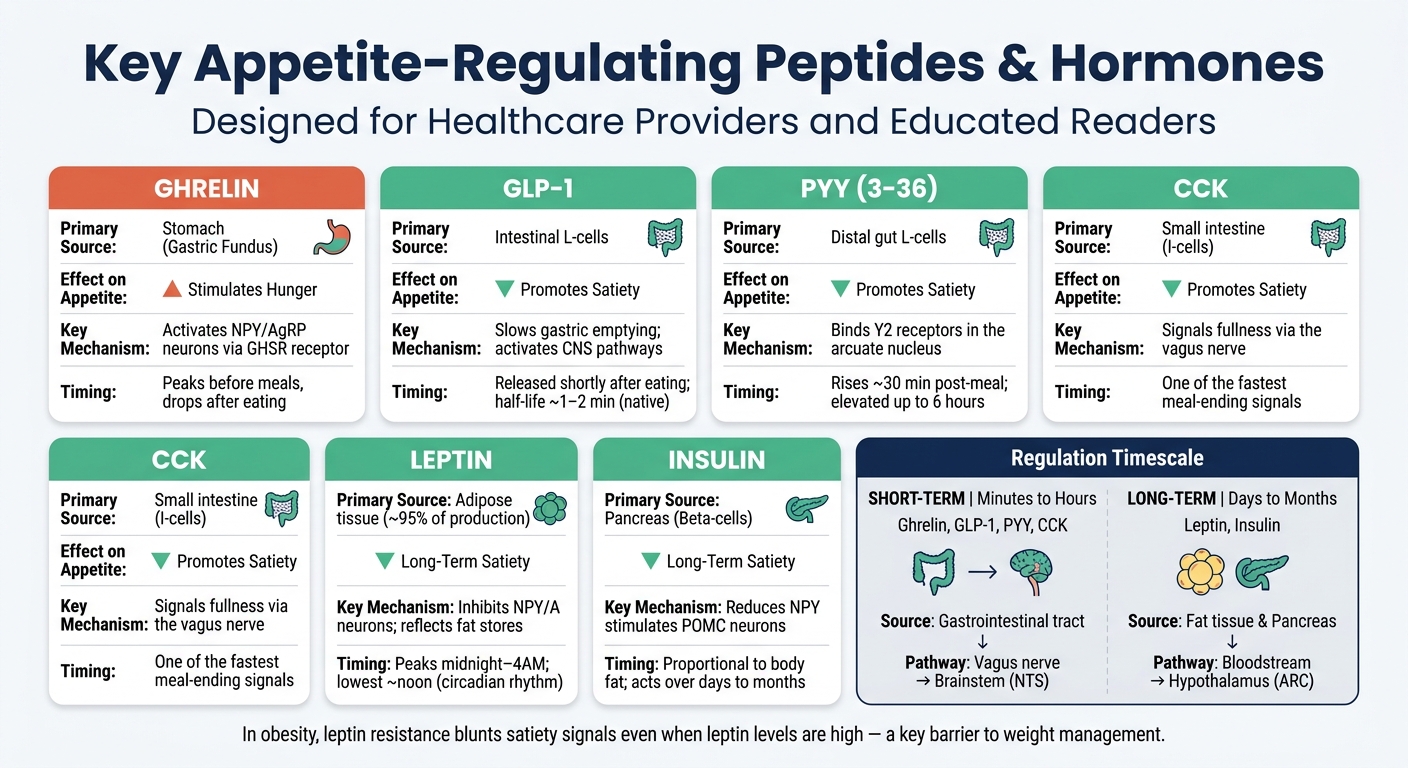
Key Appetite-Regulating Peptides: Sources, Effects & Mechanisms
The conversation between the gut and the brain involves a fascinating array of peptides and hormones, each playing a specific role in managing hunger, fullness, and energy balance.
Ghrelin: The Hunger Hormone
Ghrelin, a 28-amino acid peptide, is primarily produced in the stomach's gastric fundus and stands out as the only known peripheral hormone that actively drives appetite. It works by activating the growth hormone secretagogue receptor (GHSR), which stimulates NPY/AgRP neurons in the hypothalamus while suppressing POMC neurons that signal fullness. Ghrelin levels naturally rise during fasting, reaching their peak just before a meal, then drop after eating. Interestingly, only the acylated form of ghrelin - modified by the enzyme GOAT - stimulates appetite, while the des-acyl form may actually reduce food intake and delay gastric emptying. In a study lasting four weeks, a GOAT inhibitor (BI 1356225) reduced the acyl/des-acyl ghrelin ratio by over 80%, though it had minimal impact on weight or hunger.
"Ghrelin's nickname, the 'hunger hormone,' reflects its crucial role in stimulating appetite." - Igor Rubinić, Department of Basic and Clinical Pharmacology and Toxicology, University of Rijeka
GLP-1, PYY, and CCK: Signals of Fullness
GLP-1 (Glucagon-like Peptide-1) is released by intestinal L-cells shortly after eating. This peptide slows gastric emptying, encourages insulin release, and activates brain regions that regulate appetite. Since native GLP-1 has a short plasma half-life of just 1–2 minutes, longer-acting analogs like semaglutide have been developed, showing promising weight loss results in clinical trials.
PYY (Peptide YY), a 36-amino acid peptide, is co-released with GLP-1 from L-cells in the distal gut, especially after meals rich in protein. Its active form, PYY(3-36), targets Y2 receptors in the arcuate nucleus to suppress hunger signals. PYY levels rise within about 30 minutes of eating and can stay elevated for up to six hours.
"Proteins are the most effective macronutrient for decreasing or inhibiting food intake compared to lipids and carbohydrates." - Anaís Ignot-Gutiérrez et al., Nutrients
CCK (Cholecystokinin) is secreted by I-cells in the small intestine in response to dietary fats and proteins. It acts quickly, signaling fullness through the vagus nerve, making it one of the body's fastest mechanisms for ending a meal.
Leptin and Insulin: Regulating Long-Term Energy Balance
While ghrelin and gut-derived peptides handle short-term appetite cues, leptin and insulin oversee long-term energy regulation.
Leptin, a 167-amino acid protein, is mainly produced by adipose tissue, which accounts for about 95% of its production. It reduces appetite by suppressing NPY/AgRP neurons and activating POMC neurons. Leptin levels follow a circadian rhythm, peaking between midnight and 4:00 AM and reaching their lowest point around noon. However, in cases of obesity, persistently high leptin levels can lead to leptin resistance, blunting its effectiveness.
Insulin, secreted by pancreatic beta-cells, also contributes to long-term satiety. It crosses the blood–brain barrier to reduce NPY activity and stimulate POMC neurons, helping regulate food intake over extended periods.
| Peptide/Hormone | Primary Source | Effect on Appetite | Key Mechanism |
|---|---|---|---|
| Ghrelin | Stomach (Gastric Fundus) | Stimulates hunger | Activates NPY/AgRP neurons via GHSR |
| GLP-1 | Intestinal L-cells | Promotes satiety | Slows gastric emptying; activates CNS pathways |
| PYY(3-36) | Distal gut (L-cells) | Promotes satiety | Binds Y2 receptors in the arcuate nucleus |
| CCK | Small intestine (I-cells) | Promotes satiety | Signals via the vagus nerve |
| Leptin | Adipose tissue | Long-term satiety | Reflects fat stores; inhibits NPY/AgRP neurons |
| Insulin | Pancreas (Beta-cells) | Long-term satiety | Reduces NPY and stimulates POMC neurons |
These peptides and hormones work together in intricate ways, forming a communication network that plays a critical role in how the gut and brain coordinate appetite and energy use.
How Peptides Signal Through the Gut–Brain Axis
Understanding how peptides communicate with the brain - and how the brain interprets these messages - is central to unraveling their role in regulating appetite and metabolism.
The Role of the Vagus Nerve in Appetite Signaling
The vagus nerve acts as the main communication link between the gut and the brain. After a meal, peptides bind to specific receptors on vagal afferent neurons (VANs). These neurons, rooted in the nodose ganglia, have fibers that extensively connect to the gastrointestinal tract. Each peptide has its own receptor: CCK binds to CCK1 receptors, GLP-1 activates GLP-1 receptors, PYY3–36 targets Y2 receptors, and ghrelin interacts with GHSR receptors. Once these receptors are activated, the vagal afferents send signals to the nucleus of the solitary tract (NTS) in the brainstem, which processes nutritional information.
Interestingly, some peptides bypass the vagus nerve altogether. For example, at pharmacologic levels, GLP-1 and leptin can directly act on circumventricular organs like the Area Postrema, which lack a complete blood-brain barrier. This shows just how adaptable this signaling system can be.
"Rapid communication between the gut and the brain about recently consumed nutrients regulates metabolism and feeding behavior, both of which are critical for bodyweight maintenance." - Lisa R. Beutler, Department of Medicine, Northwestern University
Endogenous GLP-1 primarily influences meal structure through vagal pathways. However, pharmacologic GLP-1 receptor agonists, such as semaglutide, work differently by directly affecting the brainstem and hypothalamus to drive weight loss. These signals eventually converge in the brain, where areas like the hypothalamus and reward systems decode the messages.
How the Hypothalamus and Reward Pathways Process Peptide Signals
Once the vagal afferents deliver their signals, central brain structures take over to manage both basic appetite control and the pleasure-driven aspects of eating. The arcuate nucleus (ARC), situated near the median eminence where the blood-brain barrier is incomplete, detects circulating hormones directly. Within the ARC, two key groups of neurons play opposing roles: NPY/AgRP neurons trigger hunger, while POMC/CART neurons promote feelings of fullness. Remarkably, about 95% of NPY-positive cells in the ARC also express AgRP. Signals from the ARC then influence other brain regions, such as the PVN, Lateral Hypothalamus, and Ventromedial Hypothalamus.
Beyond basic appetite regulation, these peptide signals also affect the brain's reward centers. For instance, ghrelin enhances dopamine activity in the Ventral Tegmental Area (VTA) and Nucleus Accumbens (NAc), increasing the allure of calorie-rich foods. On the flip side, activating GLP-1 receptors in these same reward regions reduces the desire for highly palatable foods and curbs the motivation to seek them out.
"The effect of gut peptide receptor activation extends beyond simple homeostatic food intake control; hedonic mechanisms governing appetite are also modulated." - Jo E. Lewis, Wellcome Trust – MRC Institute of Metabolic Science
This dual impact - on both physical hunger and the emotional pull toward food - highlights how peptide-based therapies can help manage weight. For a deeper look at these mechanisms, see our clinical overview of peptide therapy. By reducing calorie intake and curbing food cravings, these treatments address both the physiological and psychological aspects of overeating.
What Human Studies Show About Peptides and Appetite
Findings from Controlled Feeding Studies
Recent research highlights how peptides influence appetite regulation, offering clear evidence from human trials. One standout study tested a "GOP" protocol - a triple-hormone infusion combining GLP-1, oxyntomodulin (OXM), and PYY. In obese participants, this combination reduced total food intake by 32% over a 10.5-hour period compared to a saline control.
"Energy intake was reduced by 32% during 10.5 hours of GOP infusion compared with 0.9% saline." - Tricia Tan, Professor of Metabolic Medicine & Endocrinology, Imperial College London
The study's results were striking. Participants consumed 468.3 kcal at lunch versus 645 kcal with saline, and 420 kcal at dinner compared to 664.7 kcal - a daily reduction of 421.1 kcal. The hormone levels achieved during the infusion mirrored those typically seen after Roux-en-Y gastric bypass (RYGB) surgery.
Interestingly, this combination therapy outperformed single-peptide treatments at lower doses. For instance, achieving a similar 21%–37% reduction in food intake using GLP-1 alone required a much higher dose (12 pmol/kg/min) compared to the triple combination (4 pmol/kg/min GLP-1 and 0.4 pmol/kg/min PYY). This underscores the effectiveness of combining peptide dosing protocols for appetite control.
Another key finding from controlled studies is the weakened satiety response in individuals with obesity. These individuals tend to have lower fasting PYY levels and a less robust post-meal PYY response. In fact, they need nearly double the caloric intake of lean individuals to achieve comparable PYY levels. This hormonal imbalance explains why traditional dieting often fails - biological signals actively resist efforts to reduce food intake.
Brain Imaging Research on Appetite and Peptides
Neuroimaging studies add another layer to our understanding of peptides and appetite by showing how these hormones influence brain activity. GLP-1 receptor agonists, for example, don’t just slow digestion - they also alter how the brain perceives food.
A study published in Science in July 2024 pinpointed GLP-1 receptor neurons in the dorsomedial hypothalamus (DMH) as critical for preingestive satiation - the feeling of satisfaction that occurs before or during eating. When GLP-1 receptor agonists were administered to patients with obesity, researchers observed increased DMH neuron activity, correlating with heightened preingestive satiation.
"GLP-1 receptor agonists are highly successful medications for obesity that are linked to shifts in food cognition, including diminished hypothalamic responses to food cues and alterations in the perception of food palatability in humans." - Peter Stern, Editor, Science
Further imaging studies have shown how peptides impact the brain's reward and addiction circuits, including areas like the ventral and dorsal striatum, amygdala, orbitofrontal cortex (OFC), and prefrontal cortex (PFC). For example, leptin replacement therapy in individuals with genetic deficiencies visibly altered brain responses to food-related visual cues, particularly in striatal regions.
Emerging techniques like manganese-enhanced MRI (MEMRI) have revealed that neuronal activity in areas like the arcuate nucleus can occur before changes in food intake. These insights help refine how clinicians approach peptide-based therapies, emphasizing their potential to reshape appetite regulation and reward pathways. Together, these findings highlight the growing role of peptides in clinical weight management strategies. For more clinical insights on metabolic medicine, stay updated with recent research.
Clinical Use of Peptides in Weight Management
Using Peptide Therapy to Control Appetite
Peptide therapy has emerged as a promising tool in weight management by targeting the body’s natural signaling pathways. These therapies work through mechanisms like slowing gastric emptying, enhancing feelings of fullness via vagal signals, suppressing hunger in the brain, and reducing the reward response to food. Addressing multiple pathways simultaneously has been shown to yield better, longer-lasting results than focusing on just one.
This approach is particularly helpful for individuals who struggle with traditional dieting. When calorie intake drops, the body often triggers a “starvation response,” where hunger hormones like ghrelin increase and satiety hormones like leptin decrease. Peptide therapy can counteract this response, making it more effective than relying solely on willpower.
Different classes of peptides have demonstrated varying levels of success. For example, GLP-1 receptor agonists such as semaglutide (2.4 mg weekly) leverage satiety and delayed gastric emptying to achieve an average weight loss of 15–20% over 68 weeks. Meanwhile, tirzepatide, a dual GLP-1/GIP agonist, has shown even greater results. In the SURMOUNT-1 trial, participants on a 15 mg dose experienced an average weight loss of 22.5% over 72 weeks, with 63% of them losing at least 20% of their body weight. Triple agonists like retatrutide, which combine GLP-1, GIP, and glucagon pathways, have demonstrated approximately 22% weight reduction at 48 weeks in Phase II trials.
| Peptide | Mechanism | Avg. Weight Loss |
|---|---|---|
| Semaglutide (GLP-1 RA) | Enhances satiety, delays gastric emptying | 15–20% |
| Tirzepatide (GLP-1/GIP) | Synergizes satiety and fat metabolism | 22.5% |
| Retatrutide (Triple Agonist) | Combines GLP-1, GIP, and glucagon | ~22% at 48 weeks |
Dose titration is a key part of therapy. For example, tirzepatide treatment typically starts at 2.5 mg weekly, increasing by 2.5 mg every 4 weeks up to a maximum of 15 mg. This gradual increase helps reduce side effects like nausea and gastrointestinal discomfort. Additionally, pairing peptide therapy with 1.2–1.6 grams of protein per kilogram of body weight daily and resistance training can help preserve lean muscle mass. Without these measures, muscle loss can account for 25–40% of the total weight lost during GLP-1 therapy.
Clinicians must also be vigilant about potential risks. Rare but serious side effects include pancreatitis and gallbladder disease, and GLP-1-based treatments should not be used in patients with a personal or family history of medullary thyroid cancer. Given that obesity is a chronic condition, long-term treatment planning is crucial. Studies show that patients may regain about two-thirds of their lost weight within a year of stopping semaglutide, emphasizing the need for sustained management.
Clinical Resources for Peptide Prescribers: PeptidePrescriber
Implementing peptide therapy safely and effectively requires access to reliable resources. PeptidePrescriber is designed specifically for licensed healthcare providers offering peptide-based treatments. The platform includes a wealth of tools such as evidence-based peptide monographs, dosing protocols, a reconstitution calculator, injection site guides, and regulatory references. Since it’s pharmacy-agnostic, practitioners can use it with any compounding pharmacy while ensuring compliance with FDA 503A/503B regulations.
For those new to peptide therapy, PeptidePrescriber also offers practical business tools like editable patient consent forms and implementation checklists. These resources make it easier for clinicians to build a peptide-focused practice without starting from scratch.
Conclusion: Applying Peptide Science in Clinical Practice
Scientific evidence leaves little doubt: appetite regulation is an intricate process governed by biological signals - a system shaped by peptides, hormones, and neural pathways that evolved to maintain energy balance. Eduardo Arilla Ferreiro from the University of Alcalá emphasizes:
"The balance between the activities of these neuronal circuits is critical to body weight regulation."
This perfectly aligns with the peptide-driven mechanisms behind hunger and fullness discussed earlier. These insights are now being translated into innovative strategies for clinical use.
For healthcare providers, this shifts the perspective on obesity. It’s not just a matter of willpower; it’s a biological challenge where hunger signals overpower those of satiety. Peptide therapies offer a pharmacological tool to recalibrate this imbalance. The most effective treatments don’t focus on a single pathway but instead target multiple points along the gut–brain axis. For instance, moving from GLP-1 monotherapy to dual and triple agonists provides broader control over metabolic processes. Additionally, studies reveal extra benefits like reduced cardiovascular risk. In fact, semaglutide has been shown to lower major cardiovascular events by about 20% over five years in obese patients without diabetes.
However, treatment efficacy isn’t one-size-fits-all. Factors such as genetics, age, sex, metabolic health, and gut microbiota composition all play a role in how well a therapy works. Following established dosing guidelines, monitoring protocols, and screening for contraindications remain critical to success. These ongoing advancements highlight how peptide science is becoming an integral part of daily clinical practice.
The landscape is rapidly changing. Oral peptide formulations, multi-receptor agonists, and deeper insights into the microbiota–gut–brain connection are expanding the possibilities for treatment. For clinicians, staying informed is no longer optional - it’s essential to providing effective, up-to-date care.
FAQs
What’s the difference between short-term and long-term appetite signals?
Appetite regulation relies on both short-term and long-term signaling systems to manage hunger and energy balance.
Short-term signals - like CCK, GLP-1, PYY, and ghrelin - kick in quickly during and after meals. These signals help control hunger and feelings of fullness on a meal-to-meal basis. Meanwhile, long-term signals, such as leptin and insulin, provide the brain with information about the body’s overall energy reserves. This feedback helps maintain weight and energy balance over extended periods.
How do gut peptides reach and affect the brain?
Gut peptides affect the brain using two primary pathways: humoral and neural.
In the humoral pathway, enteroendocrine cells in the gut release peptides into the bloodstream. These peptides can cross the blood-brain barrier and act on specific brain regions, such as the hypothalamus or the median eminence.
The neural pathway works differently. Here, gut peptides stimulate vagal afferent neurons, which send signals to the brainstem. The brainstem then communicates with the hypothalamus, helping to regulate hunger and feelings of fullness.
Why do people often regain weight after stopping GLP-1 medications?
When people stop using GLP-1 medications, weight regain often happens because these drugs are designed for long-term use rather than creating permanent metabolic changes. Once the treatment ends, appetite-regulating signals rebound, leading to increased hunger and cravings. On top of that, the body undergoes metabolic adaptation, which includes a slower resting metabolic rate and muscle loss. These changes make it harder to maintain weight. Additionally, any underlying metabolic issues typically remain, causing the body to return to its previous, higher weight over time.