
If I had to boil this down to one point, it’s this: most interaction issues with semaglutide, tirzepatide, and liraglutide come from slower stomach emptying, low blood sugar when mixed with insulin or secretagogues, and shared stomach side effects.
When applying patient selection criteria for these drugs, I’d focus first on:
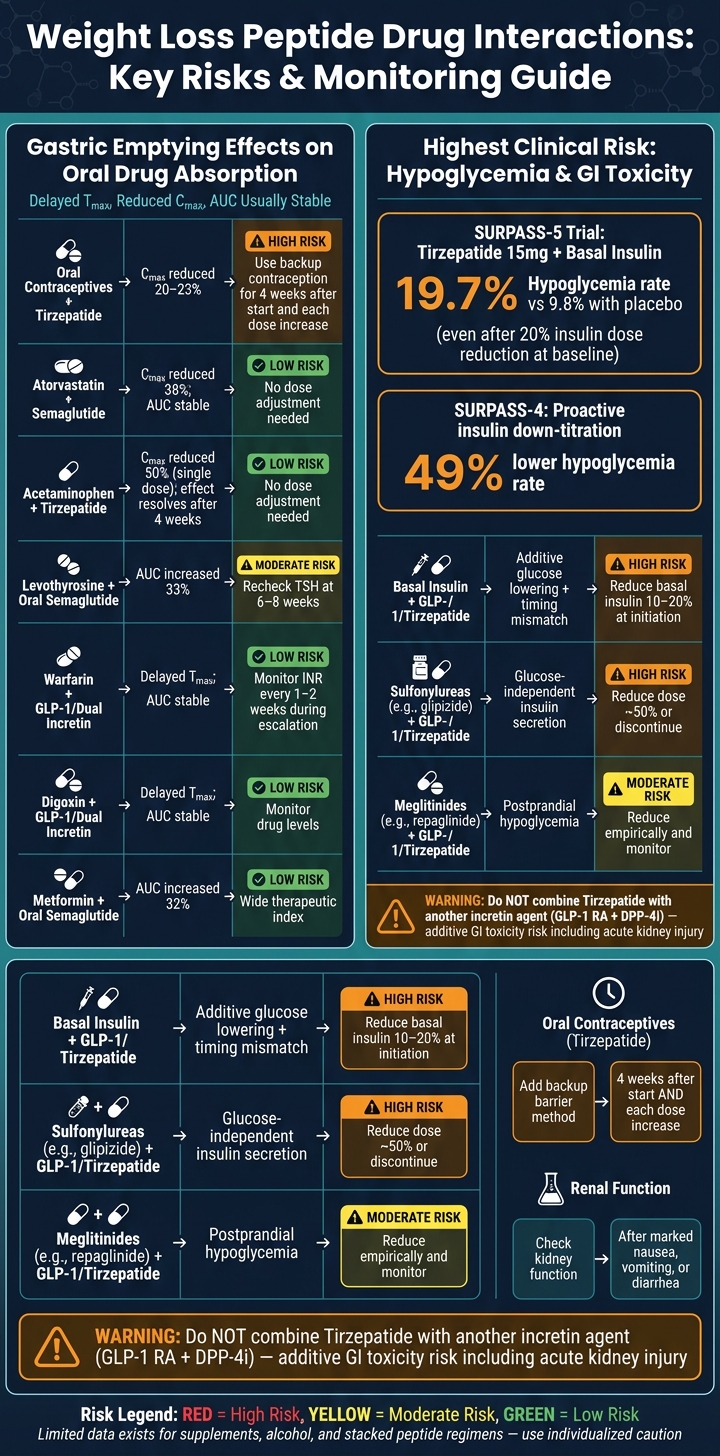
- Insulin, sulfonylureas, and meglitinides because hypoglycemia risk goes up
- Oral contraceptives with tirzepatide because absorption can drop during start-up and dose increases
- Levothyroxine, warfarin, digoxin, and other narrow-range oral drugs because timing and exposure can shift
- Nausea, vomiting, diarrhea, and dehydration because these can lead to kidney problems
A few numbers stand out:
- Tirzepatide cut oral contraceptive peak levels by about 20% to 23%
- In one study, tirzepatide cut acetaminophen C<sub>max</sub> by 50% after a single dose
- Semaglutide lowered atorvastatin C<sub>max</sub> by 38%
- With oral semaglutide, levothyroxine exposure went up 33%
- In SURPASS-5, hypoglycemia was 19.7% with tirzepatide plus basal insulin vs. 9.8% with placebo
In plain English: absorption changes are often small for many oral drugs, but blood sugar drops and GI side effects are the problems I’d watch most closely. The main action steps are simple: cut insulin or sulfonylurea doses when needed, use backup birth control with tirzepatide, recheck TSH with levothyroxine, monitor INR with warfarin, and watch hydration during bad GI symptoms.
That gives you the full picture up front, and the rest of the article fills in the study details and prescribing points. For a broader look at these treatments, see our clinical overview of peptide therapy.
Weight Loss Peptide Drug Interactions: Key Risks & Monitoring Guide
Drug interactions you should be aware of on GLP-1 medications
sbb-itb-7164bd9
What Recent Studies Show About Pharmacokinetic Interactions
These obesity peptides rarely lead to CYP or transporter drug interactions. The main PK issue is much simpler: they slow gastric emptying. When that happens, oral drugs usually absorb more slowly. In most cases, that changes the rate of absorption more than the amount absorbed. This shows up most often at the start of treatment and during dose escalation.
Delayed gastric emptying and oral drug absorption
The usual pattern looks like this: t_max goes up, C_max goes down, and AUC usually stays about the same. Recent reviews keep finding that same trend: delayed t_max, lower C_max, and AUC that usually does not change in a clinically meaningful way.
A couple of examples make that pattern easy to see. Subcutaneous semaglutide (1.0 mg) lowered atorvastatin C_max by 38%, but total AUC still stayed within acceptable limits. A single 5 mg dose of tirzepatide lowered acetaminophen C_max by 50% and delayed T_max by 1 hour. After 4 weeks of treatment, that effect was no longer seen, which suggests the gastric-emptying effect gets smaller over time. In practice, the highest-risk window is during treatment initiation and dose escalation.
The drugs that matter most here are oral therapies with a narrow therapeutic window or ones where timing of absorption matters a lot.
| Co-prescribed Drug Class | Peptide Class | Observed PK Effect | Clinical Significance |
|---|---|---|---|
| Warfarin (Anticoagulant) | GLP-1 / Dual Incretin | Delayed T_max; stable AUC/C_max |
Low; monitor INR |
| Statins (Atorvastatin) | GLP-1 / Dual Incretin | Reduced C_max (up to 38%); stable AUC |
Low; no dose adjustment |
| Digoxin (Cardiac Glycoside) | GLP-1 / Dual Incretin | Delayed T_max; stable AUC |
Low; monitor drug levels |
| Metformin (Biguanide) | GLP-1 / Oral Semaglutide | Stable AUC (SubQ); increased AUC +32% (oral) | Low; wide therapeutic index |
| Acetaminophen (Analgesic) | GLP-1 / Dual Incretin | Reduced C_max; delayed T_max; stable AUC |
Low; no dose adjustment |
| Oral Contraceptives | Tirzepatide | Reduced C_max (20–23%); delayed T_max |
High; backup method required |
| Levothyroxine (Thyroid) | Oral Semaglutide | Increased AUC (+33%) | Moderate; monitor TSH |
Oral contraceptives and other time-sensitive oral therapies
The clearest exception is tirzepatide with oral contraceptives. Because tirzepatide slows gastric emptying, it can affect oral contraceptive absorption, especially early in treatment. The label recommends using a non-oral contraceptive method or adding a barrier method for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase. Semaglutide and liraglutide do not have this restriction.
"Tirzepatide delays gastric emptying, which may impact the absorption of concomitantly administered oral medications, including oral hormonal contraceptives." - Zepbound Prescribing Information
Levothyroxine needs its own mention, especially with oral semaglutide (Rybelsus). Oral semaglutide uses the absorption enhancer SNAC and has very low bioavailability. When used together, levothyroxine exposure increased by 33%. With oral semaglutide, it makes sense to recheck TSH 6–8 weeks after starting treatment or after a therapy change. Early lab follow-up is usually more useful than changing the dose ahead of time.
The bigger clinical issue is usually additive hypoglycemia and GI toxicity, not PK change by itself.
Pharmacodynamic Interactions With the Greatest Clinical Impact
The biggest pharmacodynamic issues here are hypoglycemia and additive GI side effects. Once you’ve dealt with absorption-related effects, hypoglycemia becomes the main thing to watch.
Insulin, sulfonylureas, and meglitinides
GLP-1–based drugs and tirzepatide do not usually cause hypoglycemia on their own. The picture changes when they’re used with insulin, sulfonylureas, or meglitinides. Those pairings carry the highest risk, which is why many clinical guides suggest cutting doses early - either before peptide therapy starts or right at initiation.
The trial data make that pretty clear. In SURPASS-5, adding tirzepatide 15 mg to basal insulin led to a 19.7% hypoglycemia rate, compared with 9.8% with placebo, even though the study required a 20% insulin dose reduction at baseline. In SURPASS-4, proactive insulin down-titration under the study protocol was linked to a 49% lower hypoglycemia rate.
Sulfonylureas are often trimmed by about 50% when GLP-1 therapy begins, and some patients can stop them later as glycemic control improves. Meglitinides may need an empirical dose cut too, since weight loss peptides reduce post-meal glucose spikes. In plain terms, that can make a short-acting secretagogue unnecessary for some meals. There’s also a timing problem: delayed gastric emptying can throw off the match between mealtime insulin and carbohydrate absorption.
| Co-therapy | Interaction Mechanism | Main Outcome | Typical Clinical Response |
|---|---|---|---|
| Insulin (Basal) | Additive glucose lowering; timing mismatch with carbohydrate absorption | Increased hypoglycemia risk | Reduce dose by 10–20% at initiation; titrate based on glucose |
| Sulfonylureas (e.g., glipizide) | Glucose-independent insulin secretion | Severe hypoglycemia risk | Reduce dose by about 50% or discontinue |
| Meglitinides (e.g., repaglinide) | Short-acting insulin secretion | Postprandial hypoglycemia | Reduce empirically and monitor closely |
The other big problem is GI toxicity when incretin therapies are used together.
Combining incretin-based agents and additive GI toxicity
Tirzepatide should not be combined with another incretin-based drug because GI side effects stack. Nausea, vomiting, and diarrhea can become intense enough to cause dehydration and, in some cases, acute kidney injury.
GLP-1 RAs also should not be paired with DPP-4 inhibitors.
If you’re not stacking incretin drugs, the picture is usually simpler. Metformin and SGLT2 inhibitors tend to need only standard follow-up.
Other glucose-lowering agents with lower interaction concern
Metformin and SGLT2 inhibitors generally pose less direct interaction risk than insulin or sulfonylureas. Metformin does not cause hypoglycemia by itself, so it usually doesn’t need a preemptive dose change when a peptide is added. That said, overlapping nausea and diarrhea are common early in treatment. Taking metformin with meals may help ease that overlap.
SGLT2 inhibitors are also usually fine to use with peptide therapy. The main counseling issue is the rare risk of euglycemic diabetic ketoacidosis.
Supplements, Alcohol, and Stacked Peptide Regimens With Limited Data
Supplements that may affect glycemia, coagulation, or tolerability
The data here are thin, so the best approach is practical counseling and evidence-based guidance. Instead of looking for proven PK interactions, focus on the issues most likely to matter in day-to-day care: blood sugar, bleeding risk, and GI side effects.
Here are the supplements most worth flagging:
| Supplement | Primary Concern | Interaction Mechanism | Evidence Level |
|---|---|---|---|
| Ginseng / Ginger | Glycemia / Coagulation | May enhance hypoglycemic effects or affect platelet aggregation | Theoretical / Low |
| Chromium | Glycemia | May have additive effects on insulin sensitivity | Moderate |
| Niacin (high-dose) | Glycemia | High doses can raise blood glucose, opposing GLP-1 effects | Moderate |
| Vitamin E (high-dose) | Coagulation | May increase bleeding risk with anticoagulants like warfarin | Moderate |
For patients taking warfarin, it makes sense to step up INR checks after starting GLP-1 therapy and again after major weight loss, especially if high-dose vitamin E is in the mix.
Alcohol, dehydration risk, and gastrointestinal adverse effects
Alcohol doesn't seem to meaningfully change GLP-1 clearance, but that doesn't make it harmless in this setting. It can make nausea, vomiting, dehydration, and hypoglycemia worse.
The biggest problems are usually:
- Dehydration
- Hypoglycemia, especially in people also using insulin or a sulfonylurea
This can snowball fast. If alcohol-related fluid loss shows up at the same time as GLP-1-related GI side effects, the risk of severe dehydration and acute kidney injury goes up.
That same "limited data, focus on likely harms" mindset also applies to stacked peptide regimens.
GLP-1 therapies combined with growth hormone secretagogues
There isn't much direct human data on combining GLP-1-based therapies with growth hormone secretagogues like ipamorelin or CJC-1295. The main issue is pretty simple: GHS may reduce insulin sensitivity and push blood glucose up, which could weaken the glycemic benefit of the GLP-1 drug.
In practice, the main things to watch are glycemia, hydration, bleeding risk, and GI tolerance.
Clinical Takeaways, Monitoring Priorities, and Research Gaps
Which patients need the closest medication review
Once you get past the main PK and PD risks, the day-to-day question is simple: who needs the closest follow-up?
The patients at the top of that list are those taking insulin, sulfonylureas, or narrow therapeutic index drugs. Among these, sulfonylurea co-therapy carries the highest hypoglycemia risk. A common starting move is to reduce basal insulin by about 20% when treatment begins, then titrate based on glucose readings.
Patients taking warfarin, digoxin, levothyroxine, and tacrolimus also need closer lab follow-up, because even small changes in absorption can have clinical effects. The risk goes up in patients with gastroparesis, chronic kidney disease, or advanced liver disease, where GI losses can push kidney injury into the picture.
A full medication and supplement review should come first. From there, monitoring should match the interaction risk rather than follow a one-size-fits-all plan.
Monitoring themes consistently supported by the literature
The same interaction patterns show up again and again in the literature, and they point to a short list of monitoring priorities.
| Clinical Area | Action | Timing |
|---|---|---|
| Glucose (insulin/sulfonylureas) | Frequent checks; reduce basal insulin about 20% at start | At initiation and during titration |
| INR (warfarin) | Increase monitoring frequency | Every 1–2 weeks during dose escalation |
| TSH (levothyroxine) | Recheck thyroid function | 6–8 weeks after start or dose change |
| Oral contraceptives (tirzepatide) | Backup barrier method | 4 weeks after start and each dose increase |
| Renal function | Check renal function | After marked nausea, vomiting, or diarrhea |
Evidence is still limited for supplements, alcohol, and peptide stacking. In those areas, current guidance leans mostly on product labeling and small studies.
Conclusion: The interaction pattern clinicians should remember
The main pattern is pretty clear. Pharmacokinetic interactions with weight loss peptides are often modest. Delayed gastric emptying can change the absorption curve for oral drugs, but total exposure still tends to stay within an acceptable range for many common medications.
In practice, the bigger issues are usually pharmacodynamic: hypoglycemia, oral absorption changes, and GI or dehydration-related toxicity. That risk is highest when GLP-1–based therapies are added to insulin or secretagogues.
Tirzepatide stands out as the clearest PK exception, especially with oral contraceptives. Its labeling states that delayed gastric emptying may affect absorption of oral hormonal contraceptives, which is why backup contraception is advised during initiation and dose escalation.
Where the evidence is settled, the action steps are pretty direct: lower secretagogue doses, recheck INR and TSH, and counsel on contraception. Where the data is thin - stacked incretin regimens, supplements, and growth hormone secretagogues - the safer move is caution and an individualized review rather than assuming safety.
FAQs
Which medications need extra monitoring with weight loss peptides?
With weight loss peptides like GLP-1 receptor agonists, some people may need closer follow-up. That’s because delayed gastric emptying and fast weight loss can change how a drug is absorbed, how well it works, or when the dose should be adjusted.
The main medications to watch include:
- Diabetes medications like insulin and sulfonylureas
- Warfarin
- Levothyroxine
- Oral contraceptives
- Narrow therapeutic index drugs like digoxin, some anticonvulsants, and cyclosporine
- Antihypertensives
When should insulin or sulfonylurea doses be adjusted?
When starting weight loss peptide therapy, it makes sense to adjust insulin and sulfonylurea doses upfront to lower the risk of hypoglycemia.
For insulin, common guidance is to reduce:
- Basal insulin by 20% to 25%
- Prandial insulin by 25% to 50%
For sulfonylureas, you can either stop the drug or cut the dose by 50%, depending on the patient’s glucose pattern and overall treatment plan.
After starting therapy, step up glucose checks and make more dose changes based on blood glucose trends. This is one of those cases where a small change at the start can help prevent low blood sugar problems later.
How do tirzepatide and oral semaglutide affect other oral drugs?
Tirzepatide and oral semaglutide mainly affect other oral drugs by slowing gastric emptying. Put simply, they can make pills move through the stomach more slowly, which may delay absorption and, in some cases, change overall drug exposure.
For most medications, these effects usually aren’t clinically significant. Still, closer monitoring may be needed with narrow therapeutic index drugs such as levothyroxine, warfarin, and oral contraceptives.
With oral semaglutide, timing matters in another way too: taking it with other medications can reduce its own bioavailability by up to 50%.