Peptide targeting is about getting more drug to the heart or blood vessel lesion - and less to the rest of the body. In the article, the clearest takeaways are simple: targeting works best when the peptide matches a disease marker, the delivery system protects the payload, and clinicians watch for off-target uptake, hemodynamic effects, and product quality.
Here’s the short version in plain English:
-
Heart and vessel disease do not use the same targets.
Ischemic or failing myocardium often uses AT1 receptors or cardiac-homing peptides. Plaque, thrombus, and injured endothelium often use integrins, platelet markers, fibrin, or P-selectin. -
The point of targeting is dose efficiency and lower off-target exposure.
One preclinical study showed 3.92x higher heart concentration with AT1-targeted nanoparticles. Another found amiodarone linked to a cardiac-targeting peptide worked at 10% of the usual molar dose. -
Delivery platform matters as much as the peptide.
Free peptides are cleared fast. Nanoparticles, linkers, and pH- or redox-sensitive release systems help keep cargo intact until it reaches injured tissue. -
The biggest limits are still practical ones.
The main issues are liver/kidney uptake, manufacturing, immunogenicity, repeat dosing limits, and U.S. regulatory fit. -
Clinical review should stay simple:
check target fit, human-relevant biodistribution data, GMP quality, regulatory status, and monitoring needs.
If I were to boil the full article down to one line, it would be this: a peptide is only “targeted” when the biology, carrier, and safety plan all line up.
How Peptides Recognize Cardiovascular Tissues
Peptides localize to cardiovascular tissue by binding markers linked to disease. That selectivity is what makes targeted delivery possible.
Receptor Binding, Integrins, and Adhesion Markers on Heart and Vascular Cells
For clinicians, the practical issue is simple: which marker can you actually reach in diseased tissue? AT1, APJ, natriuretic peptide receptors, αvβ3, GPIIb/IIIa, and P-selectin are the main docking systems used in cardiovascular targeting. Common targets include AT1 receptors, APJ, natriuretic peptide receptors, αvβ3 integrins, GPIIb/IIIa on activated platelets, and P-selectin on injured endothelium.
If receptor density alone isn't enough, the tissue itself starts to offer other clues. Injury-driven permeability and changes in the matrix can give peptides another way in.
Ischemia, Inflammation, and Matrix Remodeling as Homing Signals
Myocardial capillary tight junctions limit passive drug entry. During MI, inflammatory processes and ischemia-reperfusion injury increase vascular permeability, which lets peptides and nanoparticles penetrate damaged tissue. Ischemia can also disrupt cell membranes and expose cardiac myosin on the outside of cells, where it marks injured cells.
Chronic remodeling leaves a different fingerprint. Fibroblast expansion and a collagen-based matrix network alter the extracellular matrix. Markers such as Tenascin-X (TNX) and matrix metalloproteinases (MMPs) become prominent in remodeled tissue. TNX is a primary target for CTP in remodeled cardiomyocytes. MMPs can also act as triggers for stimulus-responsive peptide-polymer systems.
Peptide Design Variables That Shape Biodistribution and Uptake
Target recognition matters only if the peptide stays intact in circulation long enough to get there. Sequence length, charge, and chemical modification shape stability, half-life, and target selectivity.
Cationic peptides like TAT (YGRKKRRQRRR) move through cell membranes well, but they also distribute non-specifically and can cross the blood-brain barrier. Cyclization, as seen with cRGD, improves conformational stability and binding affinity to integrins like GPIIb/IIIa, though it makes synthesis more complex. Disulfide linkers can keep attached cargo stable in systemic circulation while still releasing it in the reducing intracellular environment.
| Peptide Feature | Effect on Targeting | Clinical Advantage | Main Tradeoff |
|---|---|---|---|
| Cyclization (cRGD) | Increases conformational stability and affinity | Improves binding to integrins like GPIIb/IIIa | More complex and costly synthesis |
| Cationic Charge | Improves membrane penetration | High intracellular uptake | Non-specific distribution |
| Disulfide Linker | Stable in serum; cleaves inside cells | Controlled intracellular cargo release | Possible premature cleavage in some disease states |
| Sequence Length | Longer peptides can offer higher affinity | Shorter sequences are easier to incorporate onto nanoparticle surfaces | Longer sequences are harder to conjugate and synthesize |
In practice, pairing a tissue-specific peptide with a cell-penetrating peptide can help solve two problems at once. A good example is PCM combined with TAT, which can support both selective homing and efficient intracellular delivery.
sbb-itb-7164bd9
Main Cardiovascular Targeting Strategies in Clinical and Preclinical Use
Cardiovascular Peptide Targeting Strategies: Myocardial vs. Vascular vs. Receptor-Driven
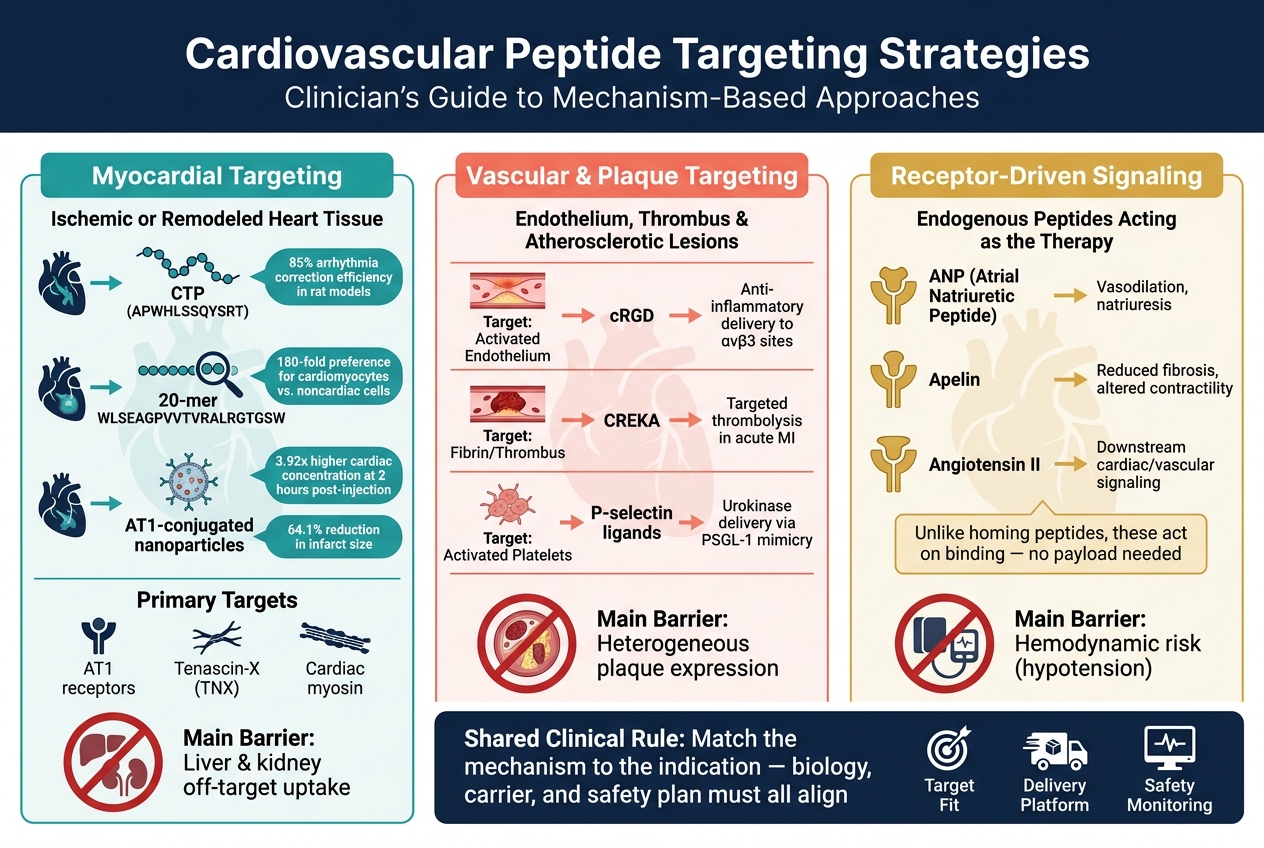
Cardiovascular peptide targeting usually fits into three main uses: myocardial delivery, vascular or plaque localization, and receptor-driven signaling. That split matters because it separates delivery problems from signaling problems.
Myocardial Targeting Peptides for Ischemic or Remodeled Heart Tissue
Myocardial targeting is about getting cargo into ischemic or remodeled heart tissue so drug levels are higher where they’re needed, while systemic toxicity stays lower.
Two cardiomyocyte-homing sequences stand out in preclinical research. The 12-amino-acid CTP (APWHLSSQYSRT) has been used to deliver imaging agents, miRNA constructs, and photosensitizers. In rat models, it restored normal heart rhythm with 85% efficiency through cell-specific rhythm ablation. The longer 20-mer WLSEAGPVVTVRALRGTGSW also showed strong selectivity, with a 180-fold preference for cardiomyocytes over noncardiac cell lines in vitro.
The AT1 peptide-conjugated nanoparticle approach pushes this idea further. In one preclinical mouse study, AT1-conjugated nanoparticles carrying anti-miR-1 reached a 3.92-fold higher cardiac concentration at 2 hours post-injection and cut myocardial infarct size by 64.1% versus MI controls.
The main barrier is straightforward: extracardiac uptake, especially in the liver and kidneys.
Vascular targeting deals with a different issue. Instead of reaching cardiomyocytes, the goal is to localize therapy to endothelium, plaque, or thrombus.
Endothelial and Plaque-Targeting Peptides in Atherosclerotic Disease
Vascular and plaque-targeting strategies try to concentrate therapy at the site of vessel injury, thrombus, or atherosclerotic lesion. The binding target depends on the clinical setting: activated integrins at injured endothelium, fibrin inside clots, and macrophage-associated receptors within plaques.
| Target Type | Example Strategy | Principal Use |
|---|---|---|
| Activated Endothelium | cRGD | Anti-inflammatory or pro-angiogenic delivery to αvβ3-overexpressed lesion sites |
| Fibrin / Thrombus | CREKA peptide | Targeted thrombolysis in acute MI |
| Activated Platelets | P-selectin-targeting ligands | Localization of thrombolytics like urokinase via PSGL-1 mimicry |
Plaques are heterogeneous, so target expression is less predictable than in myocardium. That makes vascular targeting a bit more uneven in practice.
Some cardiovascular peptides don’t just guide therapy. They are the therapy.
Endogenous Cardiovascular Peptides and Receptor-Driven Tissue Effects
Systems such as atrial natriuretic peptide (ANP), apelin, and angiotensin II bind their native receptors in cardiac and vascular tissue and trigger downstream signaling. Those effects can include vasodilation, reduced fibrosis, altered contractility, or natriuresis. That’s a different setup from homing peptides like CTP, which have no pharmacological activity on their own and need a payload to do anything.
Endogenous peptide analogs start acting as soon as they bind the receptor. But that also means their risk profile is tied to where those receptors are found across the body, including hemodynamic effects such as hypotension with ANP analogs or apelin-based constructs.
The overlap between these two models shows up in receptor-mediated nanoparticle uptake. ANP-conjugated nanoparticles and AT1-directed constructs both use the endogenous receptor as an entry point, mixing the targeting role of a native ligand with the cargo-delivery role of an engineered platform. And because a native ligand may also function as the drug, formulation and hemodynamic safety get harder to manage.
Delivery Systems, Translation Barriers, and Safety in U.S. Practice
How Delivery Platforms Improve Localization and Intracellular Delivery
Once a peptide target is identified, the next big issue is delivery. The platform decides how much intact drug gets to the target and how much is lost on the way. Free systemic peptides break down fast and are cleared fast too. Proteolysis and renal clearance sharply limit how much reaches the target site.
Nanoparticles smaller than 100 nm can move across vascular and cellular barriers and carry cargo into cells. That size matters, but surface design matters too. When the nanoparticle surface is coated with multiple targeting peptides, binding gets stronger through multivalent interactions. A single free peptide simply can't do that as well. Once bound, the interaction can trigger receptor-mediated endocytosis, which pulls the payload into the cell.
Release timing also gets better with the right carrier. pH-sensitive systems, such as calcium phosphate nanoparticles, stay stable at physiologic pH 7.4 but release cargo in the acidic microenvironment of a failing myocardium, around pH 5.5–6.5. That's the kind of switch you want: stable in circulation, active where the tissue is under stress.
Route of delivery changes the picture as well. Inhaled CTP-modified calcium phosphate nanoparticles under 50 nm move cargo from the lungs to the bloodstream and then into the myocardium fast, with maximum myocardial signals seen within 1 hour. By comparison, IV injection reaches that peak at 3 hours.
These gains in delivery bring the main translation issues into focus: safety, manufacturing, and monitoring.
Safety Monitoring, Off-Target Risk, and Regulatory Considerations
Manufacturing at scale is still one of the biggest barriers to clinical use. Extracellular vesicles and exosomes are produced in low yields, and moving them into clinical care depends on scalable production and isolation methods, along with better ways to modify in vivo biodistribution. In plain terms, the science may work, but making enough product consistently is still hard.
Immunogenicity is another problem, especially with viral-based delivery systems. Neutralizing antibodies from prior exposure can reduce the treatable patient pool and may block repeat dosing altogether. Non-viral platforms tend to offer a better safety and manufacturing profile, though that often comes with some loss in delivery efficiency.
In U.S. practice, monitoring still needs to be tight. Clinicians should track:
- Blood pressure
- Heart rate
- Arrhythmia risk
- Renal function
- Fluid balance
- NT-proBNP
That level of follow-up isn't new. Standard drugs such as milrinone already come with risks including renal dysfunction and arrhythmias. Peptide-guided formulations may help, but they don't remove the need for close monitoring. Milrinone's 1- to 2-hour half-life in humans is why it needs continuous IV infusion.
On the regulatory side, U.S. prescribers also need to think about concurrent ARB therapy. ARBs block the same AT1 receptors used by AT1-targeted strategies, which can limit how those therapies fit into care plans. Those constraints shape how peptide therapies are used in U.S. clinical workflows.
PeptidePrescriber gives licensed healthcare professionals evidence-based peptide monographs, dosing protocols, reconstitution and unit-conversion calculators, injection guides, and regulatory quick-reference tools to support compliant prescribing in U.S. practice.
Conclusion: Key Takeaways on Cardiovascular Peptide Targeting for Clinicians
Cardiovascular peptide targeting works only when the ligand, disease marker, and delivery platform line up. If they don't, uptake tends to drift toward the liver and kidneys.
The most useful clinical rule is simple: match the mechanism to the indication. Ischemic or remodeled myocardium, endothelial inflammation, and plaque disease each have different molecular signatures, and those differences matter. The best data comes from disease-selective platforms that bind injured tissue more than healthy tissue. That's the line between a therapy that is actually targeted and a peptide that merely makes its way to the heart.
Biology isn't enough on its own. Product quality and the delivery platform shape whether a target can be used in day-to-day care. The regulatory path also shifts with the platform. Before any cardiovascular-targeted peptide approach moves into routine use in U.S. practice, clinicians should check GMP manufacturing, identity, purity, sterility, stability, and conjugation data. A peptide-nanoparticle or peptide-exosome combination is regulated differently than an unconjugated peptide, and that difference has real compliance weight.
For clinical use, the last screen is straightforward: target, evidence, quality, and regulatory status.
| Decision Domain | What to Look For |
|---|---|
| Indication fit | MI, heart failure remodeling, plaque inflammation with a known molecular signature |
| Evidence threshold | Human-relevant uptake data, off-target biodistribution, and safety results |
| Product quality | GMP documentation, identity, purity, sterility, stability, and conjugation data |
| Regulatory status | FDA approval, IND/trial authorization, or IRB-approved protocol |
| Safety monitoring | Cardiac, hepatic, renal, pulmonary, and immunologic surveillance |
The bar should remain high as the field moves forward. Use targeted peptides only when the biology, product quality, and regulatory path all support the choice.
FAQs
How do peptides know where to go in heart disease?
Peptides can target cardiovascular tissue by acting like guiding ligands. In plain English, they’re built to recognize and bind to specific molecules on cardiomyocyte membranes. That can improve how precisely therapeutic cargo gets to heart tissue.
They can also get in through receptor-mediated pathways. During conditions like myocardial infarction, changes in heart structure may make it easier for peptides to reach the infarct site and deliver treatment.
Why aren’t free peptides enough for cardiovascular targeting?
Free peptides usually fall short for cardiovascular targeting. The main problem is simple: they have low stability, they break down fast, and they don’t reach the heart well on their own. They also lack the level of specificity needed to hit cardiac tissue with steady, reliable accuracy.
There’s another issue too. Physical barriers like blood flow forces and the endothelium make it hard for these peptides to get to the heart and stay there long enough to do their job. When peptides are attached to nanoparticle carriers as targeting ligands, that changes the picture. This approach can improve binding, boost retention, and make targeting more precise.
What are the biggest safety risks with targeted peptide therapies?
The biggest risk is lack of specificity. When that happens, peptides can build up in healthy tissues and cause unintended systemic side effects. Some cell-penetrating peptides may also cross biological barriers too broadly, instead of reaching only the intended cardiovascular tissue.
There are other concerns too, including long-term stability, degradation, and the way peptide structure can affect physiological function. To deal with these risks, researchers work on better targeting and run strict safety testing, including metabolic profiling and cardiac toxicity assessment.