Tumor-targeting peptides work in one of two main ways: they either guide treatment to the tumor or act on the tumor themselves. That’s the core idea.
If I boil the article down, here’s what matters most for you:
- Targeting starts with biology. These peptides bind markers that are more common on tumor cells, tumor blood vessels, or nearby tissue.
- Selectivity depends on contrast. A target usually needs a tumor-to-normal expression ratio of about 3:1 or higher to make peptide-guided delivery workable.
- The tumor site helps switch some peptides on. Lower tumor pH (6.5–6.9), enzymes like MMP-2/MMP-9, and stromal markers like FAP can all help local action.
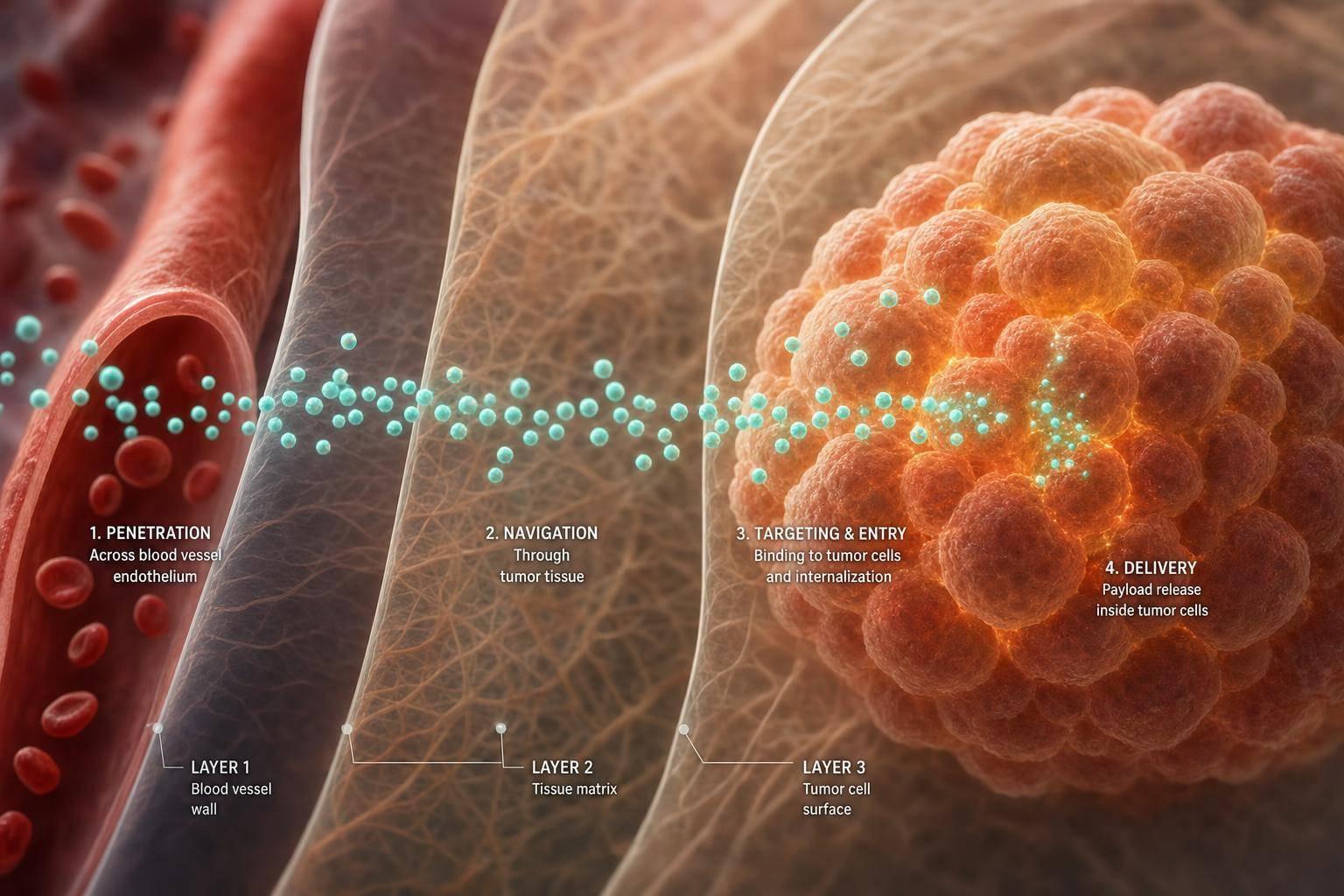
- Getting into the cell is only part of the job. Uptake route matters because it decides whether a payload reaches the cytosol, gets sent to the Golgi/ER, or ends up broken down in lysosomes.
- After localization, the peptide usually does one of four things: membrane damage, apoptosis, signaling blockade, or payload delivery.
- Clinical use depends on three checks: target expression, tumor access, and enough exposure time in the body.
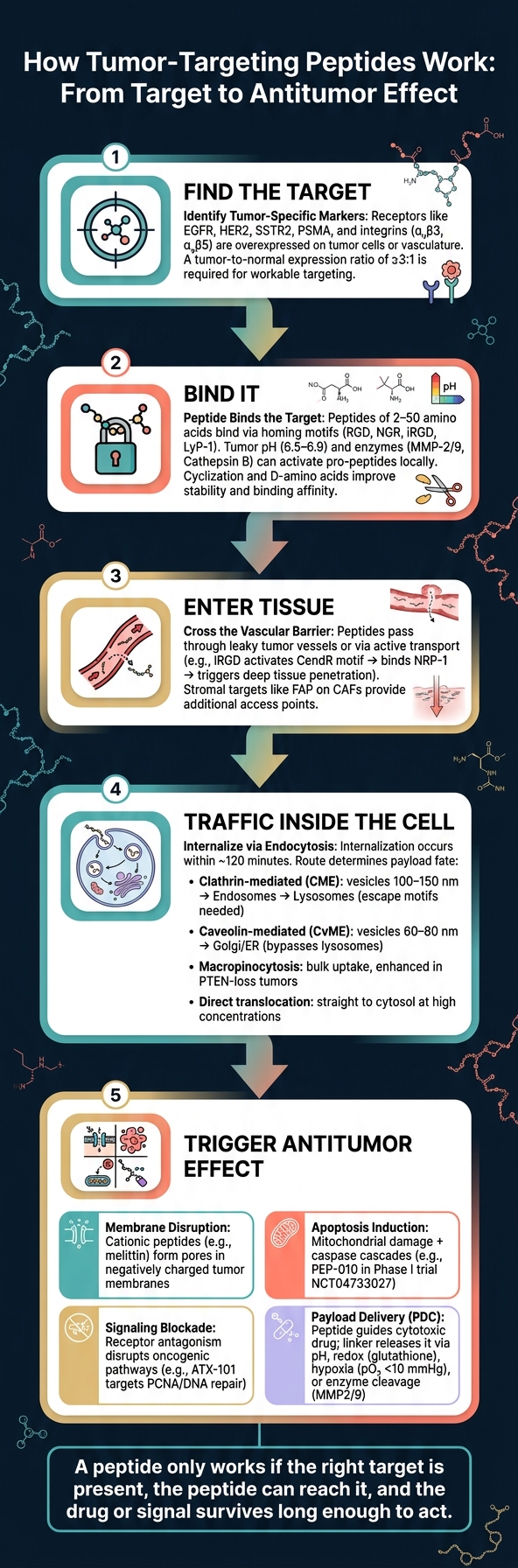
A few numbers help make this concrete. Many therapeutic tumor-targeting peptides are just 2–50 amino acids long. Internalization can happen within about 120 minutes. And some uptake vesicles differ a lot in size, such as 100–150 nm for clathrin-mediated entry versus 60–80 nm for caveolin-mediated entry.
What I take from the article is simple: a peptide only works if the right target is present, the peptide can reach it, and the drug or signal survives long enough to act. Everything else flows from that.
To make the full article easier to read, I’d frame it as a step-by-step path: find the target, bind it, enter tissue, traffic inside the cell, then trigger the intended antitumor effect.
How Tumor-Targeting Peptides Work: From Target to Antitumor Effect
Research Progress Evaluating the Function and Mechanism of Anti-Tumor Peptides
sbb-itb-7164bd9
Tumor Specificity: Receptors, Microenvironment Signals, and Targeting Motifs
Tumor specificity depends on differences between tumors and normal tissue. The big ones are receptor overexpression, abnormal blood vessels, and signals in the tumor microenvironment that healthy tissue usually doesn’t show. For targeting to be useful, you usually need a higher tumor-to-normal expression ratio. Common examples include integrins (αvβ3, αvβ5), EGFR, HER2, SSTR2, and PSMA. These three drivers - target abundance, local activation, and peptide design - set up everything that follows.
Those same differences also decide three practical things: which peptides bind, which get switched on in tissue, and which move past the vessel wall.
Tumor blood vessels are abnormal because angiogenesis happens fast and often goes wrong. That leads to marker expression such as VEGFR and CD13. Tumor pH is often 6.5–6.9, compared with 7.2–7.4 in blood, which lets pH-sensitive linkers like hydrazones release payloads at the tumor site. Enzymes such as MMP-2, MMP-9, and Cathepsin B are overexpressed in many tumors. These enzymes can cleave pro-peptides or switch on tumor-penetrating motifs like CendR. The tumor matrix is also denser and stiffer, and CAFs that express FAP add another stromal target.
Receptor Targets and Tumor-Homing Motifs
The motifs below show how these specificity mechanisms play out in practice.
RGD (Arg-Gly-Asp) binds αvβ3 and αvβ5 integrins on tumor vasculature, but its tissue penetration is limited. iRGD goes a step further. It first binds αv integrins and then, after proteolytic cleavage in the TME, exposes the CendR motif (R/KXXR/K). That exposed motif can bind Neuropilin-1 (NRP-1) and trigger active transport into extravascular tissue. In healthy organs, where those tumor proteases are not present, this penetration signal stays masked.
| Motif | Target | Main Use | Key Limitation |
|---|---|---|---|
| RGD | αvβ3, αvβ5 integrins | Tumor vasculature targeting and imaging | Limited to the vascular surface |
| NGR | CD13 (Aminopeptidase N) | Delivery of cytokines (TNF-α) and chemotherapy | Can deaminate to isoDGR, shifting its target to integrins |
| iRGD | αv integrins + NRP-1 | Deep tumor penetration and drug delivery | Requires proteolytic activation to expose the CendR motif |
| CendR | Neuropilin-1 (NRP-1) | Enhancing tissue penetration | Rapidly inactivated by plasma carboxypeptidases if unmasked |
| LyP-1 | p32 (gC1qR) | Targeting lymphatics and hypoxic tumor areas | Requires specific sequence context |
| GE11 | EGFR | Targeted nanocarrier delivery | Effectiveness depends on EGFR expression levels, which vary by patient |
Physicochemical Features That Influence Peptide Specificity
Specificity is not just about the target. It also depends on the peptide itself - its charge, stability, shape, and length all affect binding and retention.
Cationic peptides tend to favor the negatively charged membranes of cancer cells. Cyclization can improve serum stability and binding affinity because it reduces conformational flexibility. Adding D-amino acids helps peptides resist enzymatic degradation and may extend circulation half-life. Length matters too, with most therapeutic TTPs falling in the 2–50 amino acid range.
A major problem is tumor heterogeneity. Receptor expression can vary from one region of a tumor to another, and it can also differ a lot between patients. That’s why radiolabeled PET/SPECT peptides can be useful before treatment: they help confirm whether the target is actually present.
These features shape whether a peptide binds, moves through tissue, or gets into cells. Once binding happens, the next step is receptor engagement, uptake, and intracellular trafficking.
From Binding to Entry: Receptor Engagement, Tumor Homing, and Cellular Uptake
Once a peptide finds its target, binding alone isn't enough. What happens next depends on how long the peptide stays in circulation and how it gets into the tumor. Plasma proteases can break peptides down, and the kidneys can clear them out fast, so stability has a direct effect on delivery. For clinicians, understanding practical guides for handling and storage is essential to maintaining this stability. From there, peptides may pass through leaky tumor vessels or move across by active transport. Then they bind receptors and enter cells.
Receptor Binding, Tumor Vasculature, and Biodistribution
Tumor endothelium is often the first checkpoint a peptide meets. It's both a barrier and, in many cases, an early binding site. That matters because intravenously given peptides can reach receptors on the vessel surface before they ever need to move deep into tumor tissue.
It's also worth separating affinity from avidity. Affinity describes the strength of one binding interaction. Avidity is the combined strength from multiple binding interactions. In practice, multivalent peptide designs can improve avidity and help prevent the peptide from letting go too soon. That slower dissociation can increase tumor retention and support internalization. For GPCR targets like hY1R and the ghrelin receptor, rapid receptor recycling can also help by allowing repeated rounds of payload uptake.
As a rule of thumb, a tumor-to-normal-cell receptor expression ratio of at least 3:1 is usually needed before a target is seen as workable for peptide-guided delivery.
| Target Class | Biodistribution Pattern | Key PK Consideration |
|---|---|---|
| Integrins (αvβ3, αvβ5) | Tumor vasculature and angiogenic vessels | Proteolytic activation enables penetration beyond the vascular surface |
| GPCRs (SSTR2, hY1R) | Neuroendocrine and breast tumors | Rapid receptor recycling allows continuous payload shuttling |
| Growth factor receptors (EGFR, HER2) | Epithelial-origin tumors | Non-mitogenic binding avoids triggering downstream signaling |
| Stromal/TME targets (FAP, p32) | CAFs, lymphatics, hypoxic niches | Targets the tumor's supportive ecosystem to break stromal barriers |
| Transmembrane targets (PSMA, TfR) | Prostate cancer cells; blood-brain barrier | TfR ligands facilitate receptor-mediated transcytosis across the BBB |
After binding at the vessel wall or cell surface, the next issue is entry. A peptide can land on the right receptor and still fail if its uptake route sends the payload to the wrong place.
Endocytosis Pathways and Intracellular Trafficking
Once a peptide binds its receptor on the cancer cell surface, internalization can happen within 120 minutes. The uptake pathway shapes where the peptide goes next: it may stay near the membrane, get trapped in endosomes, or reach the cytosol and organelles. That routing often decides whether the payload remains intact long enough to do its job.
Clathrin-mediated endocytosis (CME) is the main route. In this pathway, vesicles about 100–150 nm wide bud from the membrane and fuse with early endosomes. Those endosomes then acidify and mature into lysosomes. That's a problem for unprotected payloads, which may be degraded before they act. To deal with that, researchers often use pH-sensitive linkers or histidine-rich endosomal escape motifs so the drug can be released before lysosomal breakdown.
Caveolin-mediated endocytosis (CvME) takes a different path. Its vesicles are smaller, around 60–80 nm, and they often avoid the lysosomal route by trafficking toward the Golgi or endoplasmic reticulum. That can help when the cargo is fragile, such as siRNA or protein-based payloads.
| Uptake Pathway | Intracellular Destination | Likely Therapeutic Consequence |
|---|---|---|
| Clathrin-mediated (CME) | Early/Late Endosomes → Lysosomes | High-volume delivery; endosomal escape motifs needed to protect payload |
| Caveolin-mediated (CvME) | Caveolin-mediated vesicles → Golgi/ER | Bypasses lysosomes; protects sensitive cargo |
| Macropinocytosis | Macropinosomes | Bulk endocytic uptake; often enhanced in PTEN-loss tumors |
| Direct translocation | Cytosol | Immediate bioavailability; typically requires high peptide concentrations |
Macropinocytosis deserves separate attention. Some tumors, especially those with PTEN loss, upregulate this pathway to a marked degree. That can make it a useful route for larger nanoparticle systems or co-administered drugs. Direct translocation, by contrast, skips the endocytic machinery and moves straight to the cytosol, but it usually needs higher peptide concentrations to work.
In short, intracellular routing is a design choice, not just a side effect. Where the peptide travels inside the cell shapes its downstream antitumor action.
Core Mechanisms of Action After Tumor Localization
Once a peptide reaches the tumor and gets taken up, its mechanisms of action typically fall into one of four categories: it damages the cell membrane, disrupts signaling, slows blood vessel growth, or carries a drug into the tumor.
Direct Antitumor Effects: Membrane Disruption, Apoptosis, and Signaling Interference
One big reason some peptides work is simple chemistry. Tumor cell membranes carry more negative charge than healthy cell membranes, so cationic peptides such as melittin are drawn in more strongly. After binding, they can form pores and destabilize the lipid bilayer.
Peptides can also kill cancer cells from the inside by triggering apoptosis. They do this by damaging mitochondria and setting off caspase cascades. PEP-010, a 30-amino acid dual-action peptide, works by disrupting the Caspase-9/PP2A interaction. In preclinical PDX models of triple-negative breast cancer, it induced apoptosis and is currently being evaluated in a Phase I clinical trial (NCT04733027).
Another direct route is signaling disruption. Some peptides act as receptor agonists or antagonists and interfere with oncogenic pathways. ATX-101, a cationic peptide that targets Proliferating Cell Nuclear Antigen (PCNA), disrupts DNA repair. It has completed a Phase I trial (NCT01462786) with a favorable safety profile and is now moving into Phase I/II trials for ovarian and peritoneal cancer (NCT04814875).
Antiangiogenic and Immunomodulatory Actions
Peptides don't just attack tumor cells. They can also make the tumor setting less supportive of growth.
One path is blocking the VEGF/VEGFR axis, which helps tumors build new blood vessels. ALM201, an FKBPL-based peptide, targets both angiogenesis and cancer stem cells in ovarian cancer models.
Peptides can also shift immune behavior inside tumors. Some modulate CSF-1R signaling and push tumor-associated macrophages toward an M1-like phenotype. BL-8040, a CXCR4 antagonist peptide, was used in the COMBAT trial with pembrolizumab and chemotherapy in pancreatic cancer to help reshape this setting. Other peptides target checkpoints and can restore T-cell activity.
Peptide-Drug Conjugates and Multifunctional Delivery Platforms
Sometimes the peptide isn't the main weapon. Sometimes it's the delivery guide.
Peptide-drug conjugates (PDCs) combine a tumor-homing peptide, a linker, and a cytotoxic payload. The idea is straightforward: use the peptide to get the drug where it needs to go, then release it inside the tumor. In TNBC models, a hydrazone-linked PDC increased intratumoral doxorubicin delivery and reduced off-target exposure compared with free drug.
The linker matters a lot because it controls where and when the payload comes off. Different linker types respond to different tumor conditions:
- Disulfide linkers are redox-sensitive and are cleaved by intracellular glutathione.
- Hypoxia-responsive linkers such as 2-nitroimidazole release payloads in low-oxygen tumor regions where pO₂ drops below 10 mmHg.
- Enzyme-cleavable linkers that respond to MMP2/9 or Cathepsin B add another layer of selectivity.
This is a useful way to separate peptide-based approaches that can look similar at first glance:
| Feature | Peptide Therapeutics | Peptide-Drug Conjugates (PDCs) | Peptide-Decorated Delivery Systems |
|---|---|---|---|
| Primary Function | Direct biological effect (agonist/antagonist) | Targeted delivery of cytotoxic payload | Guidance for nanoparticles or exosomes |
| Components | Bioactive peptide sequence | Peptide + Linker + Small molecule drug | Peptide + Nanocarrier (liposome/NP) |
| Mechanism | Signaling inhibition, membrane disruption | Intracellular drug release after uptake | Enhanced accumulation and cell entry |
| Complexity | Low | Moderate | High |
| Example | Foxy-5, Melittin | 177Lu-DOTA-TATE, PE-EGF | iRGD-labeled liposomes, GE11-Exosomes |
Clinically, that distinction matters because the same peptide scaffold can act as the drug itself, the carrier, or both, influencing patient selection criteria for these therapies. Those categories set up the clinical framework in the next section.
Clinical Translation: Mechanism-Based Interpretation and Key Takeaways
What works in the lab doesn't always work in the clinic. At the bedside, peptide use comes down to three simple checks: target expression, tissue access, and exposure time.
Start with receptor expression. If a target doesn't show a meaningful tumor-to-normal ratio, the odds of selective benefit drop fast.
But strong expression alone isn't enough. Tumors have physical barriers, and those barriers can limit how far a drug moves once it gets in. That's one big reason some receptor-positive patients still don't respond.
Then there's stability. Peptides are broken down fast in plasma and lysosomes, so half-life extension is often needed to keep exposure long enough to matter.
A Mechanism-Based Framework for Evaluating Peptide Regimens
Use this sequence to judge whether a peptide regimen is likely to work in a given tumor:
- Identify the target: Is the receptor - SSTR2, PSMA, EGFR, hY1R - overexpressed in this patient's tumor type at a clinically meaningful ratio?
- Classify the peptide by function, not by scaffold alone: Is it working as an active agent through direct signaling inhibition or membrane disruption, or as a vector that delivers a cytotoxic payload as a PDC?
- Define the uptake route: Does it rely on clathrin-mediated or caveolin-mediated endocytosis? Clathrin-mediated uptake is faster, but it can push the peptide toward lysosomal degradation. Caveolin-mediated uptake avoids lysosomes, though cargo release may be slower.
- Match the downstream effect to the tumor's biology: Line up the mechanism - antiangiogenic, pro-apoptotic, or immunomodulatory - with the patient's tumor stage and microenvironment profile.
- Match PK/PD to dosing and monitoring: Look at serum stability and circulation time when setting the dosing schedule. Then pair monitoring with the mechanism: PET or SPECT for target engagement, MRI or near-infrared imaging for vascular effects, and CD8+ T-cell or IL-6 changes for immune activity.
FAQs
How do tumor-targeting peptides find cancer cells?
Tumor-targeting peptides home in on cancer cells by binding to receptors, antigens, or biomarkers that show up at much higher levels on tumor cells and in the tumor microenvironment.
These peptides are designed or picked to recognize those molecular signals with high affinity. That helps them gather at the tumor site instead of drifting into healthy tissue. After binding, many are pulled into the cell through endocytosis, which can help deliver therapeutic or diagnostic payloads.
What makes one peptide enter cells differently than another?
Peptides get into cells in different ways, and a lot of that comes down to their biochemical traits. Things like amino acid sequence, charge, polarity, and hydrophobicity shape how a peptide behaves once it reaches the cell surface.
In practice, these traits help decide whether a peptide binds to overexpressed receptors and gets pulled inside through endocytosis, or works as a cell-penetrating peptide that moves across membranes more directly.
On top of that, synthetic modifications can improve delivery, stability, and controlled release. That can make a big difference when the goal is to help a peptide last longer, reach the right cells, and release at the right time.
Why do some tumor-targeting peptides fail in patients?
They can fail for a pretty simple reason: they don't stay intact long enough to do the job.
Many are biologically unstable, which means they have a short half-life due to rapid excretion and protease degradation. On top of that, clinical use can be held back by poor targeting selectivity, weak tissue penetration, and overall systemic instability.
To deal with this, researchers are testing chemical modifications that improve stability, along with delivery platforms built to boost therapeutic efficacy.