
Chondroinductive peptides are transforming cartilage repair. These short amino acid chains stimulate chondrogenesis, helping stem cells become cartilage-producing cells. Unlike growth factors, they’re more stable, less likely to trigger immune responses, and easier to integrate with biomaterials. This makes them a promising option for addressing cartilage damage and osteoarthritis (OA), which affects over 595 million people globally.
Key Takeaways:
- What They Do: Promote cartilage formation by activating pathways like SOX9 for hyaline cartilage production.
- Why It Matters: Articular cartilage heals poorly, and current OA treatments only manage symptoms without repairing damage.
- Clinical Advances:
- Delivery Challenges: Peptides face hurdles like rapid clearance and limited penetration in joints, but solutions like collagen-binding peptides and nano-in-gel systems improve retention and effectiveness.
Researchers are advancing these therapies to address unmet needs in orthopedic care, providing hope for better cartilage regeneration solutions.
Mechanisms and Classes of Chondroinductive Peptides
Growth Factor-Derived Peptides
These peptides replicate critical regions of natural signaling proteins, such as TGF-β and BMPs, without delivering the entire protein. They interact directly with transmembrane receptors on mesenchymal stem cells (MSCs), triggering signaling pathways that promote cartilage formation.
Take CK2.1 as an example. This peptide, which mimics BMP receptor type Ia, initiates chondrogenesis at just 100 nM while avoiding hypertrophy - a common issue with the full BMP-2 protein that can lead to unwanted calcification.
"CK2.1 drives chondrogenesis and cartilage formation without the induction of chondrocyte hypertrophy, suggesting its use as a promising therapeutic tool for cartilage-degenerative diseases." - Maria Giovanna Rizzo et al., University of Messina
Another standout is the BMP7-derived peptide p[63–82]. Research published in Arthritis Research & Therapy by Maastricht University in 2025 highlights its cyclic variant, C2. At concentrations as low as 0.001 nM, C2 not only increased collagen type 2 expression but also reduced inflammatory markers like PTGS2 and MMP-13, outperforming its linear counterpart.
Now, let’s shift focus to peptides that replicate extracellular matrix (ECM) cues.
ECM- and Adhesion-Derived Peptides
Unlike growth factor-derived peptides, ECM- and adhesion-derived peptides act more as a scaffold. They mimic structural signals found in the extracellular matrix, helping cells attach, survive, and cluster into cartilage-forming groups.
The RGD sequence (Arg-Gly-Asp) is a well-known example. Found in fibronectin, laminin, and other matrix proteins, RGD binds integrin receptors on cells, anchoring them and supporting matrix deposition. Another peptide, GFOGER, mimics collagen and interacts with α1β1 and α2β1 integrins, promoting chondrogenic differentiation.
N-cadherin mimetic peptides, particularly those with the HAV motif, play a crucial role in simulating cell-to-cell interactions seen during embryonic limb development. These interactions drive mesenchymal condensation, a necessary step for chondrogenesis. Without this condensation, differentiation cannot proceed.
Key Mechanisms of Action
These peptide classes work through distinct, yet complementary, mechanisms. Here’s a breakdown:
Table: Peptide Classes and Mechanisms
| Peptide Class | Key Examples | Signaling Pathway | Primary Effect |
|---|---|---|---|
| TGF-β Mimetics | CM-1, HSNGLPL | SMAD2/3 | Early MSC differentiation; ECM synthesis |
| BMP Mimetics | CK2.1, p[63–82] (C2) | SMAD1/5/8 | Chondrogenic differentiation; anti-hypertrophy |
| ECM-Derived | RGD, GFOGER | Integrin (α1β1, α2β1) | Cell attachment; matrix deposition |
| Adhesion-Derived | HAV, HAVDI | N-cadherin | Mesenchymal condensation; early chondrogenesis |
In addition to receptor binding, these peptides combat cartilage breakdown. For instance, BMP mimetics like p[63–82] suppress markers of hypertrophy, such as COL10A1, and reduce enzymes like MMP-13 that degrade cartilage. This dual action - boosting matrix formation while inhibiting degradation - is particularly promising for treating osteoarthritis.
"The p[63–82] peptide has unique suppressive actions on the hypertrophic and mineralizing OA chondrocyte phenotype." - Arthritis Research & Therapy
Peptide cyclization further enhances their stability and activity in arthritic joints. Cyclic variants, such as C2 of p[63–82], maintain their effectiveness even at lower doses.
These mechanisms highlight the therapeutic potential of chondroinductive peptides in cartilage repair and regeneration.
Clinical Applications and Use Cases
Osteoarthritis and Cartilage Defects
Osteoarthritis is a widespread issue, but current treatments only manage symptoms without actually repairing damaged cartilage. Chondroinductive peptides are changing this by addressing the disease directly at the cartilage level.
Take LNA043, a peptide derived from ANGPTL3 and developed by Novartis. In a Phase 1 double-blind trial (NCT02491281) involving 28 patients with knee osteoarthritis, a single intra-articular injection of LNA043 achieved impressive results. It penetrated damaged cartilage 4 times deeper than healthy cartilage in the same joint and reversed osteoarthritis-related gene expression for at least 21 days. These results are tied to the peptide's ability to activate critical cartilage-regenerating pathways.
"LNA043 is a novel disease-modifying OA drug candidate that... reverses the OA transcriptome signature over at least 21 d, inducing the expression of hyaline cartilage matrix components." - Nature Medicine
By 2022, LNA043 advanced to a Phase 2b trial (NCT04864392). Similarly, TPX-100, developed by OrthoTrophix Inc., completed Phase 2 trials (NCT01925261) for patello-femoral osteoarthritis, showing lasting improvements in both knee function and cartilage structure. These developments signal a shift toward disease-modifying osteoarthritis drugs (DMOADs) - treatments focused on regenerating cartilage instead of just reducing pain.
While direct injection therapies are making strides, they’re also paving the way for scaffold-based approaches that use peptides to create environments conducive to cartilage repair.
Scaffold-Based Regeneration
Peptides are also being integrated into biomaterial scaffolds to enable in situ cartilage repair. These scaffolds are designed to recruit the patient’s own mesenchymal stem cells (MSCs) and guide their transformation into cartilage-producing chondrocytes - eliminating the need for cell transplantation.
At Dalian Medical University, researchers developed a promising example by grafting CM10 (LIANAK) peptides onto functional nanofibrous hollow microspheres (FNF-HMS). When implanted in mice, this scaffold led to significant cartilage formation, with strong glycosaminoglycan (GAG) and collagen deposition and minimal calcification. A key benefit of covalently bonding peptides to scaffolds, rather than simply mixing them into hydrogels, is their durability - allowing for a longer-lasting influence on cartilage matrix production.
"Synthetic chondroinductive biomaterials might be the answer to the unmet clinical need for a safe, stable, and cost-effective material capable of inducing true hyaline cartilage formation." - Tissue Engineering Part B: Reviews
While scaffold-based techniques focus on regeneration, peptide therapies are also being explored for sports-related cartilage injuries.
Orthopedic and Sports Medicine Applications
Sports injuries, such as ACL tears and medial meniscal tears (MMT), often lead to posttraumatic osteoarthritis (ptOA), which can progress quickly in younger, active individuals. Chondroinductive peptides are being studied as a potential solution for these cases.
For example, BMP7-derived peptides have shown promise in preclinical studies. The peptide p[63–82] was tested in rat models of ACL transection and partial medial meniscectomy, demonstrating significant reductions in joint degeneration scores and improved weight-bearing capacity at 5 and 10 weeks. Importantly, these benefits were achieved without triggering hypertrophic differentiation, a common hurdle in cartilage repair.
Here’s a quick look at the current status of key peptide therapies:
| Peptide / Platform | Indication | Trial Phase |
|---|---|---|
| LNA043 (Novartis) | Knee OA / Cartilage Injury | Phase 2b Clinical Trial |
| TPX-100 (OrthoTrophix) | Patello-Femoral OA | Phase 2 Clinical Trial |
| p[63–82] | Posttraumatic OA (ACL/Meniscus) | Preclinical (Rat Models) |
| PEDF 29-mer | MIA-Induced OA | Preclinical (Rat Models) |
As these peptide-based therapies continue to progress through advanced clinical trials, orthopedic and sports medicine specialists will need to stay informed to determine how and when these treatments can be effectively incorporated into patient care.
Can peptides repair articular cartilage?
sbb-itb-7164bd9
Peptide Delivery and Localization Strategies
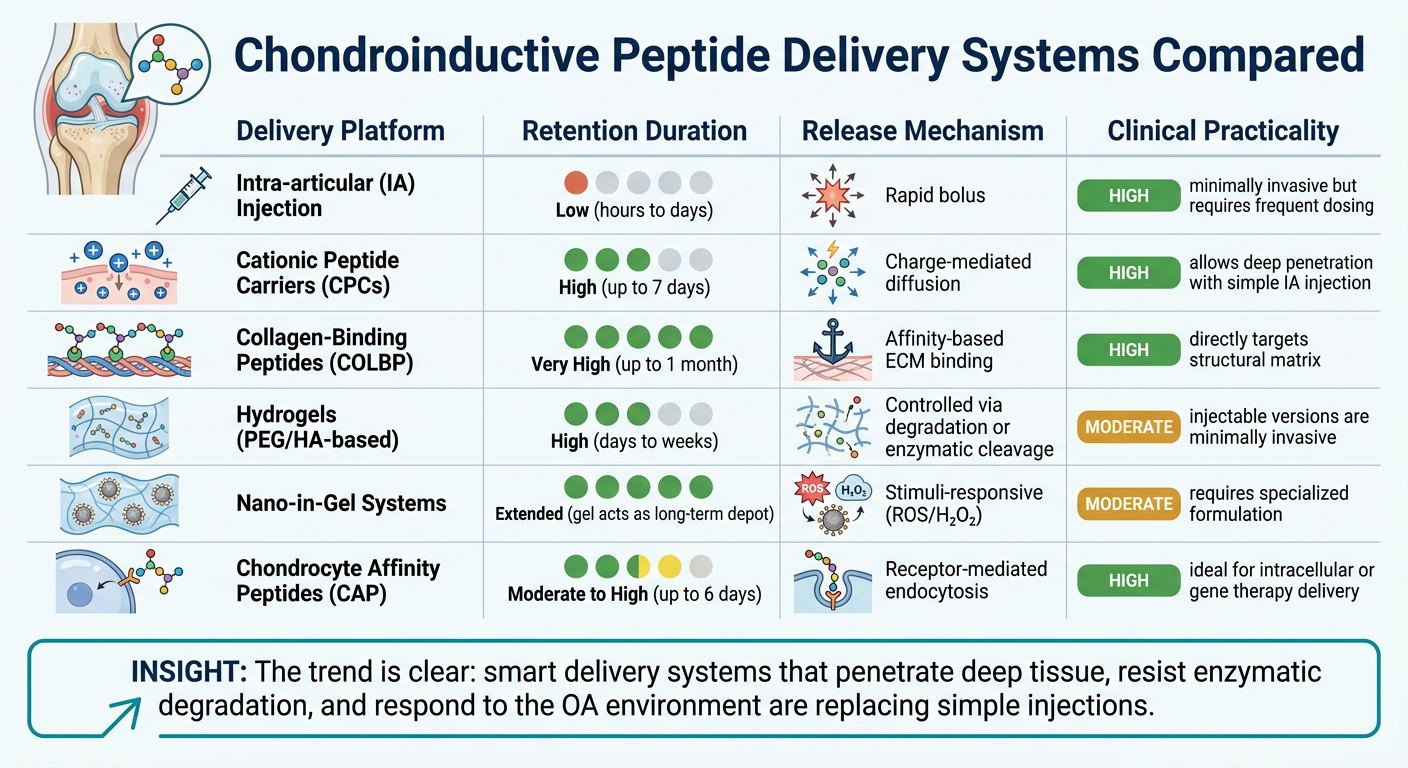
Chondroinductive Peptide Delivery Systems: Retention & Clinical Practicality Compared
Getting a chondroinductive peptide into a joint is one thing. Ensuring it stays in the cartilage long enough to make a difference is another. Cartilage, being avascular and lacking lymphatics and nerves, is practically unreachable by systemic drugs. Add to that the dense, negatively charged cartilage matrix, which acts as a physical barrier, and the challenge becomes even greater. Without a targeted delivery approach, even the most carefully designed peptide can be cleared from the joint within hours, making specialized delivery systems essential for effective cartilage targeting.
"IA administration offers improved local bioavailability... However, its pharmacokinetics are limited by rapid joint clearance, competitive binding with SF, enzymatic degradation, and restricted penetration through dense extracellular matrices." - npj Biomedical Innovations
Biomaterial-Based Delivery Systems
To tackle these obstacles, biomaterial-based delivery systems have emerged as key players. Cationic peptide carriers (CPCs) use charge interactions to penetrate the negatively charged cartilage matrix. Research shows that these carriers can retain detectable levels for up to 7 days after a single intra-articular injection. Additionally, CPC-modified imaging agents have achieved equivalent cartilage CT signals at doses 40 times lower than unmodified agents.
Another approach involves collagen-binding peptides (COLBP), such as WYRGRL, which anchor directly to the triple-helix domains of Type II collagen. This method ensures stable retention, with collagen-binding avimers (~4 kDa) demonstrating localization in rat knees for up to a month after a single injection. For applications requiring both deep tissue penetration and sustained release, nano-in-gel systems present a promising solution. These systems encapsulate small targeting nanoparticles within a hydrogel, which serves as a depot, gradually releasing the nanoparticles in response to the oxidative stress environment characteristic of osteoarthritis.
Challenges in Cartilage Localization
Even with advanced delivery systems, cartilage localization faces significant hurdles. Synovial proteases degrade peptides before they can reach their target, and competitive binding with synovial fluid components further reduces the amount of bioavailable peptide. Neutral or negatively charged carriers encounter an additional challenge: the cartilage matrix’s negative charge actively repels them, making uptake difficult. The solution often lies in combining charge-based targeting with structural protection. For example, encapsulating peptides within nanoparticles or covalently bonding them to scaffolds can dramatically improve their durability and sustained activity - both critical for achieving cartilage regeneration.
Comparison of Delivery Platforms
Here’s a quick look at how different delivery methods stack up:
| Delivery Platform | Retention | Release Mechanism | Clinical Practicality |
|---|---|---|---|
| Intra-articular (IA) Injection | Low (hours to days) | Rapid bolus | High; minimally invasive but requires frequent dosing |
| Cationic Peptide Carriers (CPCs) | High (up to 7 days) | Charge-mediated diffusion | High; allows deep penetration with simple IA injection |
| Collagen-Binding Peptides (COLBP) | Very high (up to 1 month) | Affinity-based ECM binding | High; directly targets structural matrix |
| Hydrogels (PEG/HA-based) | High (days to weeks) | Controlled via degradation or enzymatic cleavage | Moderate; injectable versions are minimally invasive |
| Nano-in-Gel Systems | Extended; gel acts as long-term depot | Stimuli-responsive (ROS/H₂O₂) | Moderate; requires specialized formulation |
| Chondrocyte Affinity Peptides (CAP) | Moderate to high (up to 6 days) | Receptor-mediated endocytosis | High; ideal for intracellular or gene therapy delivery |
The trend is unmistakable: moving beyond simple injections toward smart delivery systems that can penetrate deep into tissue, resist enzymatic degradation, and respond to the pathological environment for precise, sustained release.
Clinical Translation and Practice Considerations
From Preclinical to Clinical Use
Turning preclinical successes into effective clinical applications presents a significant challenge. Much of peptide research is still conducted in in vitro settings. As highlighted in Tissue Engineering Part B: Reviews:
"Clinical translation of peptides will require the evaluation of these peptides in well-controlled in vivo cartilage defect studies."
There are, however, some promising examples of progress. OrthoTrophix Inc. conducted Phase 2 randomized, double-blind, placebo-controlled trials (NCT01925261 and NCT02837900) between 2017 and 2018 for TPX-100, a peptide derived from matrix extracellular phosphoglycoprotein. This study targeted mild to moderate patellar osteoarthritis. Similarly, Samumed LLC (now Biosplice Therapeutics) initiated a Phase 3 multicenter trial (NCT04385303) in July 2020 for Lorecivivint (SM04690), a Wnt pathway inhibitor, focusing on patients with moderately to severely symptomatic knee osteoarthritis. While these trials signal progress, they also highlight the need for more standardization and regulatory efforts before these therapies can see broader clinical adoption.
One of the key technical obstacles is the "hypertrophy gap." This refers to the tendency of differentiated chondrocytes to shift toward a hypertrophic phenotype, characterized by Type X collagen production and alkaline phosphatase activity. This shift often leads to apoptosis and matrix mineralization, rather than effective cartilage repair. Currently, engineered cartilage tissue achieves only about 50% of the collagen content found in native cartilage.
While advancements in trials are encouraging, ensuring both efficacy and safety remains a priority.
Safety and Evidence Quality
From a safety perspective, chondroinductive peptides present some clear advantages over recombinant growth factors. These peptides are chemically synthesized, which ensures higher purity, better batch-to-batch consistency, and a reduced risk of immunogenicity. For instance, unlike BMP-2 - which can lead to hypertrophy and calcification - CK2.1 has been shown to promote hyaline cartilage formation. It increases collagen types II and IX without inducing Type X collagen or mineralization. Remarkably, CK2.1 achieves these effects at concentrations as low as 100 nM, similar in efficacy to 40 nM of the full BMP-2 protein.
However, clinicians need to critically evaluate the evidence, as most studies are still in the preclinical phase. Key considerations include whether the peptide supports a true hyaline cartilage phenotype instead of fibrocartilage, whether the delivery system ensures controlled, sustained release without an initial burst, and whether it has been rigorously tested in well-controlled in vivo defect models.
Supporting Clinicians with PeptidePrescriber
Given the complexities of peptide therapy, clinicians benefit from reliable tools to guide their practice. PeptidePrescriber is designed to meet this need, offering evidence-based peptide monographs, standardized dosing guidelines, regulatory updates, and practical tools like reconstitution calculators and injection guides. Since many chondroinductive peptides are still in the preclinical phase, this platform helps practitioners verify regulatory status and access vetted protocols, reducing the risks associated with experimental use. Importantly, PeptidePrescriber is pharmacy-agnostic, making it a valuable resource for both seasoned prescribers and those new to peptide therapies who aim to establish a well-informed, compliant practice.
Conclusion
Chondroinductive peptides present a focused and stable alternative to traditional growth factors and invasive cell-based treatments in the pursuit of hyaline cartilage regeneration - a goal that has long been a challenge in orthopedic medicine. This shift is driven by various peptide classes, each designed to target specific stages of cartilage repair.
These peptides fall into several categories, including growth factor mimetics like CK2.1, adhesion-derived sequences, and tissue-targeting peptides such as CAP and COLBP (WYRGRL). Together, they address critical steps in the repair process - from initiating chondrogenic differentiation to ensuring precise delivery to damaged tissue. As noted in Tissue Engineering Part B: Reviews:
"The search for chondroinductive compounds and materials is an emerging area of research with peptides at its heart." - Tissue Engineering Part B: Reviews
While the clinical potential is clear, the challenges are equally significant. With osteoarthritis affecting millions worldwide, the development of peptides that can integrate into biomaterial scaffolds, be delivered directly into joints, and adapt to the unique conditions of each joint holds immense promise.
For healthcare providers, staying informed is crucial. The regulatory environment for peptide-based therapies is evolving, and the gap between preclinical research and clinical application remains a hurdle. Tools like PeptidePrescriber aim to bridge this gap by offering healthcare professionals access to detailed peptide monographs, dosing protocols, reconstitution calculators, and regulatory insights - all without favoring any specific pharmacy.
Clinicians who prioritize evidence-based practices and keep pace with advancements in this field are better equipped to deliver improved outcomes as peptide therapies continue to develop.
FAQs
How are chondroinductive peptides different from growth factors like BMPs and TGF-β?
Chondroinductive peptides stand out as a promising alternative to growth factors like TGF-β and BMPs, which come with their own set of hurdles, including high costs, instability, and dilution within the body. These peptides are synthetic, which means they offer greater stability, consistent results, and improved efficiency. While BMP-2 is effective in promoting cartilage repair, it carries risks such as triggering unwanted chondrocyte hypertrophy and calcification. Specific mimetic peptides are crafted to reduce these risks, making them a safer option.
Which chondroinductive peptides are closest to FDA-approved clinical use in the U.S.?
Currently, no chondroinductive peptides have been fully approved by the FDA for clinical use in the United States. The majority of research in this area is still in the preclinical phase, concentrating on laboratory experiments and animal studies.
One potential breakthrough is LNA043, a peptide derived from angiopoietin-like 3. This candidate has already completed a phase 1 trial to evaluate its safety and pharmacokinetics in humans. It is now progressing through phase 2b trials, targeting knee osteoarthritis, as it moves further along the regulatory pathway.
What delivery method keeps peptides in knee cartilage the longest after injection?
Research indicates that cationic peptide carriers (CPCs) significantly improve peptide retention in knee cartilage. Articular cartilage is rich in negatively charged molecules, such as aggrecan-glycosaminoglycans, which interact with positively charged peptides through electrostatic forces. This interaction forms a stable drug depot, prolonging the peptides' residence time. Incorporating these carriers into hydrogels can further boost both tissue penetration and extended retention.