
One public reply can turn a bad review into a HIPAA problem. My takeaway is simple: I should use the same review process every time - triage first, draft with neutral wording, get approval, post from one account, and log what happened.
Here’s the short version:
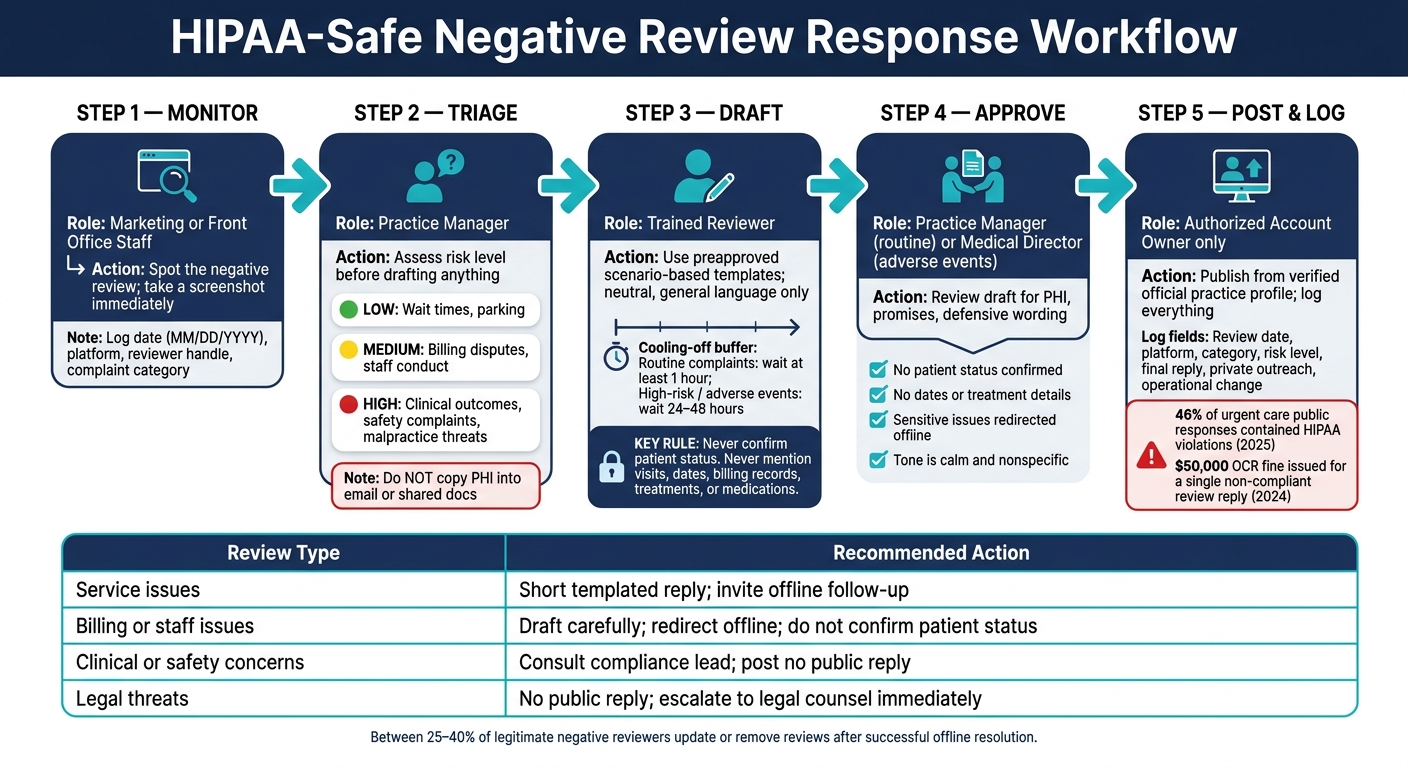
- I do not confirm that the reviewer is a patient
- I do not mention visits, dates, billing records, treatment, or medications
- I keep public replies short, neutral, and general
- I move billing, care, safety, and legal issues offline
- I use an internal log to track the review, the reply, and any follow-up
The risk is not small. The article notes a $50,000 OCR fine tied to a public review response, and one 2025 review found 46% of urgent care responses included HIPAA violations. That tells me the issue is often the reply itself, not just the review.
If I need a simple rule, it’s this: acknowledge the feedback without confirming anything, then point to a private contact method. For clinical complaints, safety issues, or legal threats, I may be better off posting no public reply at all.
This article lays out a clear process I can use to respond with less risk and more consistency.
Build a standard workflow for every negative review
HIPAA-Safe Negative Review Response Workflow for Medical Practices
An unanswered review - or a rushed one - can create both reputation problems and HIPAA risk. The fix is simple in theory: set a clinic-wide process before anyone replies in public.
Give each step to a specific role:
- Monitoring: marketing or front office staff
- Triage: practice manager
- Drafting: a trained reviewer
- Approval: practice manager or medical director
- Posting: one authorized account owner
That way, the team can move from review intake to drafting in a calm, controlled way instead of reacting on the spot.
Triage the review and gather facts internally
As soon as a negative review appears, take a screenshot. Reviews can be edited or deleted, so keeping the original version matters. Then add the review to an internal tracking document with the date in MM/DD/YYYY format, the platform name, the reviewer handle, and a complaint category such as scheduling, billing, staff conduct, communication, or clinical outcome.
Next, sort the review by risk level before drafting anything. Complaints about wait times or parking are usually low risk. Billing disputes and staff conduct issues are often medium risk. Clinical outcome or safety complaints are high risk, and any malpractice threat should be escalated inside the practice before a reply is drafted.
When the team checks the facts, they should pull the chart or billing record only inside secure systems. Keep source records there. Do not copy PHI into email, shared documents, or draft responses. If the review may involve an adverse event, pause for 24 to 48 hours, escalate to the medical director, and document the incident before writing a response.
Draft, approve, and post through assigned roles
After the facts are gathered, build in a short cooling-off period before drafting. Wait at least one hour for routine complaints and 24 to 48 hours for high-risk or adverse-event reviews. That buffer helps keep the response steady and non-emotional.
The drafter should use preapproved, scenario-based templates that speak to general practice policies, not a person’s specific experience. Have approved templates ready for each platform the clinic monitors. The practice manager can approve routine responses, while the medical director should review any response tied to an adverse event. Only the authorized account owner should publish the final reply.
Log outcomes and improve care
Every negative review, public response, and follow-up step should go into one internal document. Include the review date, platform, category, risk level, final reply, private outreach, and any operational change that followed.
This log should do more than store complaints. It should help the clinic spot patterns. If reviews keep mentioning weak injection teaching or poor results in a peptide practice, that may point to gaps in patient education or documentation. Fixing those gaps can lower the odds of similar reviews showing up again.
Resources from PeptidePrescriber can support that process with counseling guides, injection materials, and documentation tools. When a clinic tracks review patterns and ties them to operational fixes, the response process becomes repeatable and easier to defend over time.
With the workflow in place, the next step is writing a HIPAA-safe public reply.
sbb-itb-7164bd9
How to write HIPAA-safe public replies
Once your reply is drafted and approved, run it through this structure before you post it. The main rule is simple: never confirm patient status. Even a small slip in a public reply can lead to HIPAA trouble, and recent enforcement actions make that pretty clear.
How to structure a compliant response
A safe public reply usually follows a plain, repeatable pattern. Acknowledge the feedback in general terms, mention your commitment to quality care, and direct the person to a private channel like your office phone number or a secure patient portal.
Here’s a good gut check: could a stranger learn anything about the reviewer’s health, finances, or treatment from your reply? If the answer is yes, rewrite it.
That means avoiding lines like "we're sorry your visit didn't go as expected" because that confirms a visit. Skip "our billing team reviewed your file" because that confirms a financial record. And stay away from any mention of a date, medication, or procedure. This rule still applies even when the reviewer already shared those details in public.
When a short reply or no reply is the right call
For issues like wait times, parking, or front desk tone, a short template is usually the best move. For clinical outcomes, safety concerns, or legal threats, do not post a public reply. Instead, document the choice internally with a plain reason such as "Risk of PHI disclosure" or "Active legal concern," then escalate it through the right channel.
If a review includes hate speech, explicit threats, or another patient’s PHI, skip the reply and file a platform removal request. Report it under the platform’s terms of service, not medical facts.
Use the table below to match the complaint type to the right response level.
| Review Type | Recommended Action |
|---|---|
| Service issues | Short templated reply; invite offline follow-up |
| Billing or staff issues | Draft carefully; redirect offline; do not confirm patient status |
| Clinical or safety concerns | Consult compliance lead; post no public reply |
| Legal threats | No public reply; escalate to legal counsel immediately |
Compliant vs. non-compliant response examples
These examples help keep replies neutral and safe.
| Non-Compliant (Avoid) | Compliant Alternative (Use) | Why It Matters |
|---|---|---|
| "We're sorry you had a bad visit." | "We strive to provide excellent care to everyone." | Avoids confirming the reviewer was a patient. |
| "Your appointment on June 10th..." | "Our policy is to see all patients promptly." | Protects dates of service, which are PHI. |
| "We discussed your peptide therapy." | "We take all clinical concerns seriously." | Protects specific treatment and medication details. |
| "Our billing team reviewed your file." | "Please contact our office manager at [Number]." | Moves sensitive financial issues to a secure channel. |
Keep your tone professional and move sensitive issues offline
Once the wording is compliant, tone is what makes the reply feel credible. Keep in mind: the reply is public. Write for prospective patients, not for the reviewer alone. That means the tone should stay calm, neutral, and general. It should never confirm patient status or get into details about care.
The aim is simple. Sound calm and professional without saying whether the person is a patient or sharing anything about treatment. Use “we” and “our practice” instead of “you” or “your visit.” Keep the focus on the practice’s values and approach. Skip defensiveness, blame, and extra detail.
When to take the discussion offline
Take the conversation offline when a review involves an adverse event, a treatment disagreement, a billing or refund dispute, a discrimination allegation, or a legal threat. If a review is abusive, defamatory, or part of a legal dispute, a public reply may not make sense at all. In those cases, keep any public response to one or two sentences, say that privacy limits what can be shared, and give one offline contact method.
It also helps to document what happened. Log the review, the risk level, the contact person, the date, and the resolution. Between 25% and 40% of legitimate negative reviewers update or remove their reviews after a successful offline resolution, so a careful private follow-up can pay off.
Don’t reply to fake or non-patient reviews. Flag them for removal.
Before posting, review the draft for PHI, promises, and defensive wording. The next risk isn’t tone. It’s what the reply might reveal or promise by accident.
Mistakes to avoid when replying to negative reviews
Once you know the basic shape of a safe reply, the next job is simpler: don’t make the kind of mistakes that create HIPAA trouble or damage your reputation. Treat this as a last pass before anything gets posted - the final check during drafting, approval, and publishing.
Do not disclose PHI, argue publicly, or explain care decisions in detail
The first risk comes from what you say. At this point, the three biggest errors are confirming patient status, defending clinical decisions, and replying from a personal account.
The worst mistake is confirming that the reviewer was a patient. Even an apology can suggest a patient relationship, and that alone can be enough to create a HIPAA violation. Public replies should not justify a diagnosis, treatment protocol, or medication choice. And staff should never respond from a personal account. Use the verified practice profile only, so the reply stays inside the practice review process.
The penalties aren’t theoretical. In October 2024, the OCR fined a dental practice $50,000 after it replied to a negative Google review with specific details about the patient’s interaction and clinical situation.
"A covered entity may not confirm or deny that a particular person was, in fact, a patient, or disclose any other individually identifiable health information." - Office for Civil Rights (OCR)
Do not make promises, threats, or undocumented exceptions
The second risk comes from what you promise. Don’t offer a refund or billing exception in public. Move billing issues to a private channel through the office. And don’t threaten legal action in a reply. If you think a review crosses the line into defamation, send it to counsel offline and stay silent in public.
For serious complaints, route the issue through the practice manager, compliance officer, or counsel before any public response goes out.
Here’s a quick side-by-side view of the highest-risk mistakes and the safer move instead:
| Mistake | Risk | Safer Alternative |
|---|---|---|
| Confirming the reviewer was a patient | HIPAA violation, OCR fines | Use practice-wide language that addresses no one specifically |
| Defending a specific diagnosis, protocol, or medication | PHI exposure, legal risk | Reference general evidence-based standards only |
| Offering a public refund or billing exception | Undocumented precedent | Direct the person to your billing office privately |
| Threatening legal action in a reply | Reputational damage, escalation | Send defamation concerns to legal counsel offline |
| Replying from a personal staff account | Bypasses practice review | Always use the verified official practice profile |
If you reply at all, keep it brief, neutral, and nonspecific.
Conclusion: A repeatable process for responding to negative reviews
Once the reply is live, consistency is what matters most. A negative review doesn't have to turn into risk if your team follows a documented, HIPAA-safe response process that covers each step: review, draft, approval, post, and log.
A written process helps keep emotion out of public replies. In plain terms, that means triaging before anyone writes a response, keeping public replies short and nonspecific, moving sensitive matters offline, and logging each step for compliance.
That log should also help your team spot patterns worth fixing on the inside. If the same complaints keep showing up around billing, wait times, or communication, that's not just a reputation problem. It's a process signal.
The goal is simple: build a repeatable system that protects privacy, preserves trust, and keeps every response consistent.
FAQs
Can I apologize without violating HIPAA?
Yes - you can apologize without violating HIPAA, as long as the apology stays general and neutral and keeps the focus on your practice’s commitment to quality care.
What you should not do is confirm that the reviewer is a patient, mention treatment, or refer to case details - even if the reviewer already posted that information themselves.
Keep your reply brief. Then invite them to contact your office privately so you can discuss their concerns offline.
Who should approve a negative review response?
To protect HIPAA compliance and keep professional standards in place, owners or clinicians shouldn't reply directly, especially when emotions are running high. That's where things can go sideways fast. A better move is to give review responses to one trained person or a small, dedicated team.
Your process should also include review or approval from legal counsel, a privacy officer, or management when a review brings up serious clinical or legal concerns. If there's any doubt about HIPAA compliance, check with your privacy officer or legal counsel before posting.
When should we avoid replying in public?
Avoid replying in public when emotions are running high, the review touches on sensitive clinical outcomes or possible adverse events, or any reply could suggest a treatment relationship.
Don’t argue in public or try to set the record straight there. That can put PHI at risk. If the matter involves complex clinical complications, send it to the right internal team for review and shift the conversation to a secure, private channel using neutral, practice-wide language.