If I prescribe or administer a peptide that I can’t trace, I’m taking on patient risk and legal risk at the same time. The main trouble points are simple: the vial may contain the wrong drug, the wrong strength, hidden additives, or poor sterile prep. Testing reports on unregulated products found purity from 0% to 99.3%, a 78.5% median, and some vials with no detectable active peptide at all.
Here’s the short version:
- Wrong ingredient or strength can lead to treatment failure, overdosing, or bad follow-up data
- Injectable products carry extra danger because contamination and endotoxins go straight into tissue or blood
- Bad labels can lead to mg/mcg mix-ups and reconstitution errors
- Missing sterility, endotoxin, and lot records make patient care and chart support much harder
- “Research use only” labels do not protect me if the product is used in patient care
- My safest path is to verify the source, document the lot, review testing, instruct the patient in writing, and stop use when records are missing
A few numbers stand out:
- Reported peptide potency ranged from 50% to 200% of label claim
- Endotoxin reactions may start within 30 to 90 minutes
- Fever above 100.4°F after injection is a warning sign
- Fever above 101.3°F, chills, low blood pressure, or fast heart rate can point to an endotoxin reaction
| Risk area | What can go wrong | What I should do |
|---|---|---|
| Product identity | Wrong peptide, degraded drug, no active ingredient | Review lot-specific CoA and source records before first dose |
| Dose accuracy | Underdose, overdose, mg/mcg mistakes | Confirm vial strength, diluent, final concentration, and dose math |
| Sterility | Cellulitis, abscess, sepsis, tissue reaction | Require sterility and endotoxin data for injectables |
| Labeling | False or incomplete instructions | Reject vague, reused, or RUO-style labeling for patient care |
| Legal exposure | Board review, chart problems, commerce issues | Record source, lot, consent, rationale, and follow-up |
So the takeaway is plain: if the paper trail breaks, use should stop. The article below walks through the main clinical harms, the charting weak points, and the source-check steps I’d want in every clinic workflow.
Clinical Risks from Counterfeit Peptides
Wrong Ingredient, Wrong Strength, and Avoidable Treatment Failure
Once a counterfeit peptide reaches a patient, the problem is no longer just a sourcing issue. It becomes a direct clinical risk.
A vial can have the right label and still contain the wrong peptide, a degraded product, or the wrong strength. Independent testing has found wrong identity, truncated sequences, and impurities that were not listed on certificates of analysis.
What happens next depends on the type of failure. Underdosing may lead to little or no response, which can be mistaken for disease progression or poor patient adherence. Overdosing can lead to a stronger pharmacologic effect than the prescriber intended. And when treatment is tracked with objective markers - such as IGF-1 for growth hormone-axis peptides or A1c for GLP-1 agents - inaccurate potency makes follow-up data much harder to read.
Infection, Inflammatory Reactions, and Tissue Injury from Injectables
Contamination does not always show up right away. Sometimes the first few injections seem fine, and the problem appears later, when local irritation turns into cellulitis, an abscess, or a systemic infection.
There’s also a separate issue: sterile inflammatory reactions. In these cases, no live organisms are present. Instead, particulates, unstable buffers, or degraded compounds trigger local inflammation, pain, and swelling.
| Feature | Expected | Red Flags |
|---|---|---|
| Duration | Resolves within a few hours | Lasts more than 48 hours |
| Pain level | Brief stinging or mild itching | Intense pain or spreading tenderness |
| Systemic signs | None | Fever (>100.4°F / 38°C), chills, or dizziness |
| Visual cues | Minor swelling or small bump | Pus, extensive swelling, or spreading redness |
Delayed abscesses and inflammatory nodules may show up days after injection. That timing matters. These reactions are often blamed on the patient’s underlying condition instead of the product, and that wrong call can slow down the right response while the sourcing issue continues in the background.
Hidden Safety Variables: Undocumented Preservatives and Excipients
If the full ingredient list is missing, prescribers can’t properly screen for allergy risk, route compatibility, or reconstitution behavior. Residual solvents, impurities, and additives may trigger inflammation, antibody formation, or anaphylaxis.
"A COA for a non-sterile bulk powder will not include [sterility testing] - that is acceptable, but the end preparation must be tested." - PeptidePrescriber
The same sourcing failures can also throw off dosing and batch-level quality control. Misleading concentration labels and missing reconstitution instructions add another layer of risk.
sbb-itb-7164bd9
Dosing, Sterility, and Quality-Control Failures
Misleading Concentration Labels and Incomplete Reconstitution Instructions
Beyond ingredient risk, the next point of failure in peptide therapy is simple execution: dose conversion, reconstitution, and lot verification.
Even if a peptide itself is legitimate, a vague label can still put someone in harm’s way. Third-party testing has found potency ranging from 50% to 200% of the label claim, which means a calculated dose can land far above or below the intended target. One of the most common mistakes is mg/mcg confusion. That sounds small on paper, but it can change a dose in a big way.
FDA has already documented serious adverse events tied to mismeasured compounded injectable GLP-1 doses, including nausea, vomiting, and diarrhea requiring medical care. If a vial doesn’t clearly state the diluent, reconstitution volume, and final concentration, each dose becomes a guessing game.
At a bare minimum, the label should show:
- Total amount per vial
- Concentration
- Reconstitution volume
- Final concentration
- Dose per administration
Missing Sterility Assurance, Endotoxin Testing, and Batch Documentation
For injectable products, sterility and endotoxin testing aren’t optional details. They’re basic safety checks. USP <71> and USP <85> lay out sterility and endotoxin expectations, and if either one is missing, that leaves a major safety hole.
Endotoxin reactions tend to show up fast, often within 30 to 90 minutes after injection. Typical signs include chills, fever above 101.3°F (38.5°C), tachycardia, and hypotension. At higher loads, the reaction can progress to septic shock.
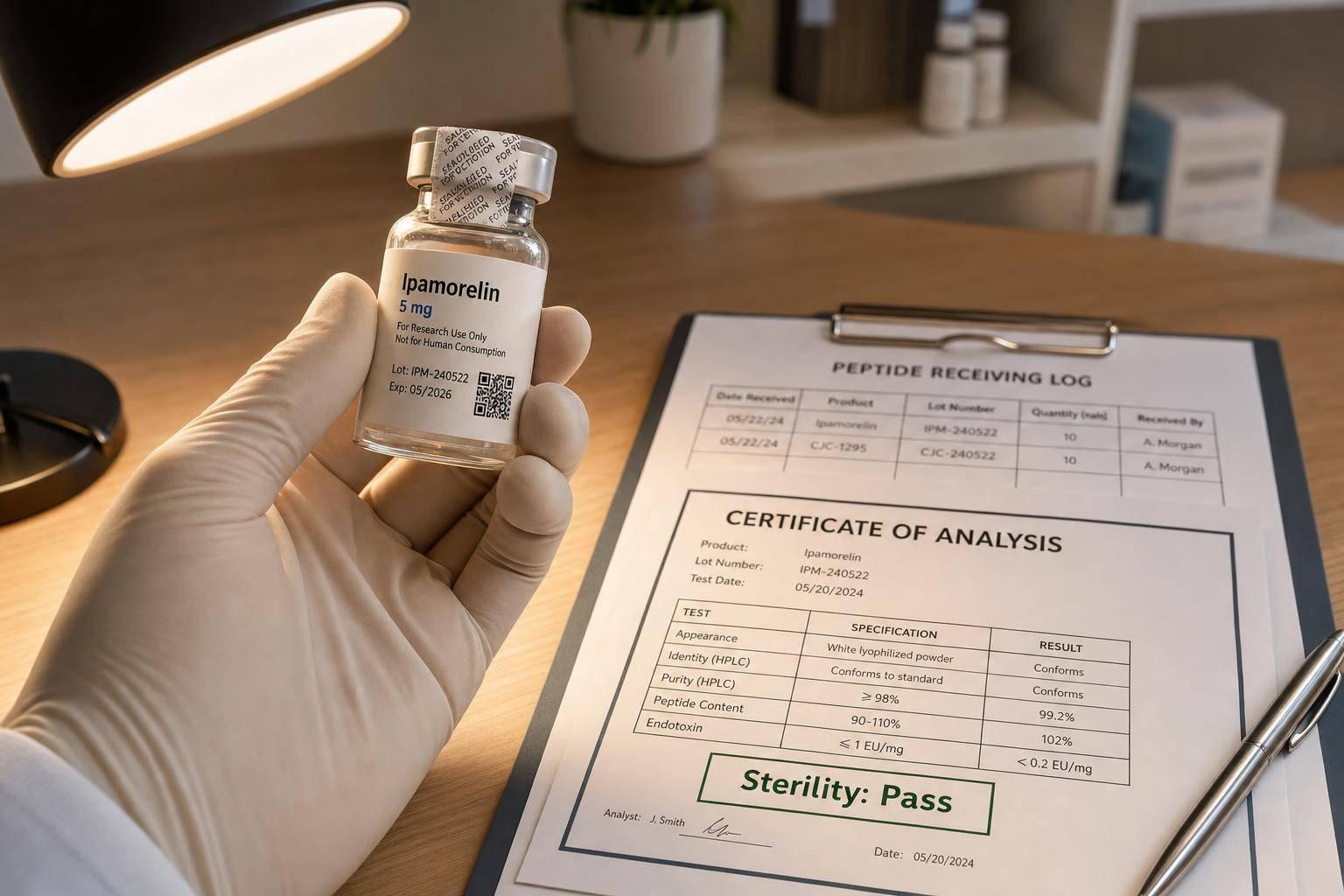
Independent testing of unregulated peptide vendors paints an ugly picture. Reported purity ranged from 0% to 99.3%, with a median of 78.5%. A large share of products contained no detectable active peptide or included undisclosed active substances. That’s not a small labeling slip. It means the vial may contain far less than expected, something else entirely, or nothing useful at all.
A lot-specific CoA should confirm:
- Identity
- Potency
- Purity
- Sterility
- Endotoxin status
- Lot number
Without that paper trail, tracing a reaction back to a specific product or lot becomes close to impossible.
Those same record gaps also create legal exposure when a bad lot needs to be tracked down.
Legal and Professional Exposure for Prescribers
Counterfeit Peptide Source Red Flags vs. Safe Sourcing Signals for Prescribers
When source records are missing or thin, a patient-safety issue can turn into a regulatory one fast. And once that happens, it can also become a legal problem.
Misbranding, Unapproved Products, and State Board Scrutiny
The FD&C Act bars the introduction of counterfeit, misbranded, or unapproved drugs into interstate commerce. For prescribers, that’s not just legal theory. If you use a product sold as research use only in actual patient care, you can step into misbranding exposure.
FDA has stepped up enforcement against compounded peptide and GLP-1 products that suggest FDA approval, claim they’re the same as approved drugs, or carry RUO labeling while being sold for clinical use.
State medical boards are moving the same way. At least one board has said publicly that physicians cannot dodge accountability through "research-grade" labeling or patient consent forms. What do boards look for? They want to see whether the chart shows deliberate source review and clear patient disclosure. In these cases, investigators usually focus on three points:
- Why the prescriber chose an unapproved product
- Whether informed consent plainly disclosed the product’s regulatory status
- Whether office policies separate FDA-approved, compounded, and non-approved products
Documentation Gaps That Weaken Your Defense
In high-risk peptide cases, the defense often falls apart for a simple reason: the prescriber can’t tie the vial to a checked source or a specific lot. A defensible chart should record the source, pharmacy license and state, lot number, expiration date, rationale, consent, and follow-up.
That’s why source verification needs to happen before the first dose, not after an adverse event.
Source Verification and Traceability Checks Before Prescribing or Administering
Before ordering any injectable peptide, confirm that the dispensing entity has a current state pharmacy license. If it’s a 503B outsourcing facility, verify current FDA registration too. Ask for a lot-specific Certificate of Analysis (CoA) with identity, purity, sterility, and endotoxin results. Make sure the product arrived with intact tamper-evident packaging, matching lot numbers, and proper cold-chain records. If a supplier can’t produce that paperwork, treat it as a stop-use signal, not a back-and-forth.
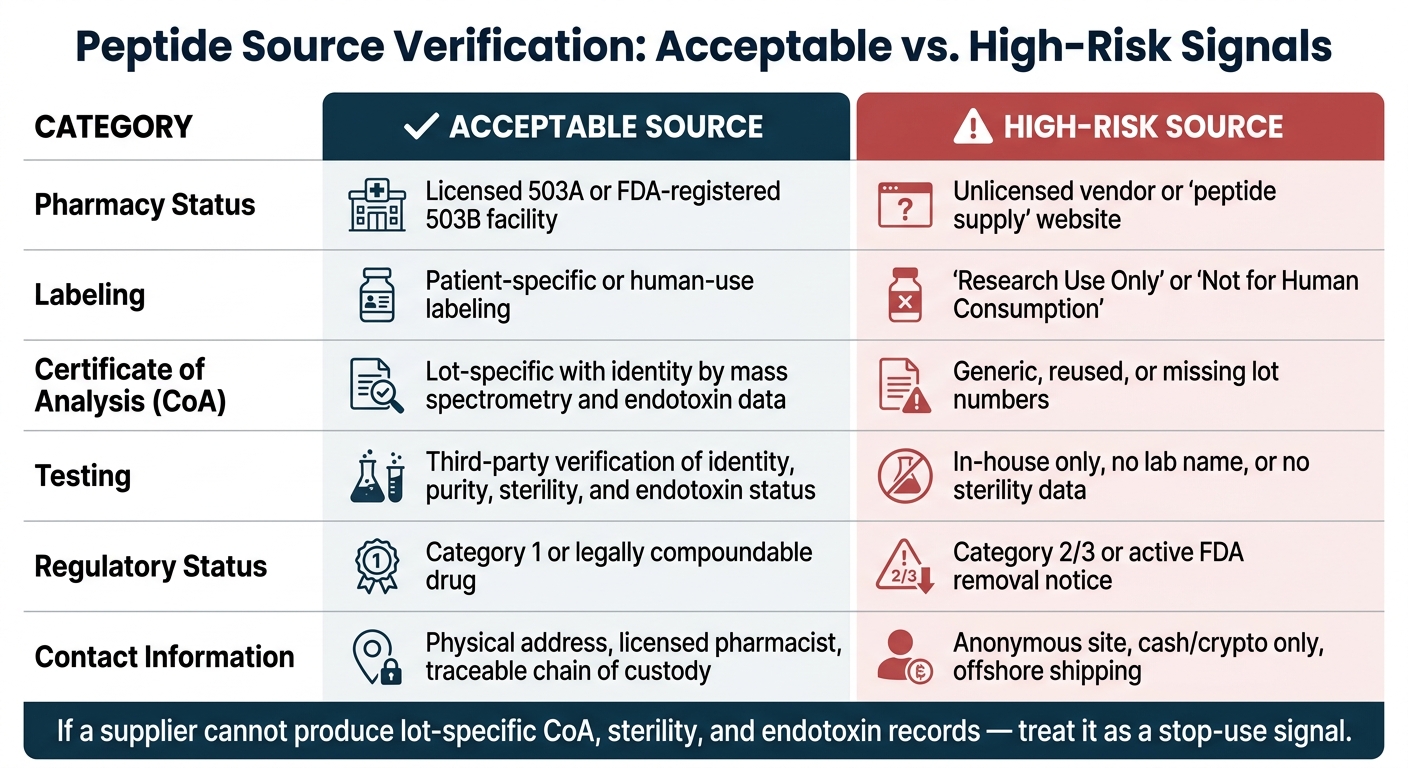
The table below shows the signals that separate acceptable sources from high-risk ones:
| Sourcing Signal | Acceptable | High-Risk |
|---|---|---|
| Pharmacy status | Licensed 503A or FDA-registered 503B | Unlicensed vendor or "peptide supply" website |
| Labeling | Patient-specific or human-use labeling | "Research Use Only" or "Not for Human Consumption" |
| CoA type | Lot-specific with identity by mass spectrometry and endotoxin data | Generic, reused, or missing lot numbers |
| Testing | Third-party verification of identity, purity, sterility, and endotoxin status | In-house only, no lab name, or no sterility data |
| Regulatory status | Category 1 or legally compoundable drug | Category 2/3 or active FDA removal notice |
| Contact information | Physical address, licensed pharmacist, traceable chain of custody | Anonymous site, cash/crypto only, offshore shipping |
Disclaimers like "for research only" don’t give legal cover when the actual use and marketing are plainly aimed at clinical use. If the vial label says one thing and the chart note says another, that mismatch can become some of the most damaging evidence in a board or malpractice review.
These checks should sit inside the standard prescribing workflow.
Prescriber Risk-Reduction Workflow and Key Takeaways
Standardize Source Review, Patient Instructions, and Adverse-Event Escalation
Once source verification is set, the next problem is simple: people don't always do it the same way. A source check only protects patients if it happens on every single order.
Put those steps into a written clinic SOP and assign clear roles for prescribing, nursing, and admin staff. On each order, require:
- source review
- written patient instructions
- adverse-event escalation when needed
If a patient has an unusual reaction or an unexpected response, stop dosing at once. Then review the lot and verify the source before starting again. Do not resume until the source is verified. Escalate through the adverse-event process.
Use Evidence-Based Tools to Support a Compliant Peptide Workflow
A written SOP is far more useful when the clinic also relies on standard templates and calculators. Keeping up with FDA, USP <797>, and state board rules is hard without a set system.
PeptidePrescriber provides evidence-based monographs, dosing protocols, calculators, injection guides, and regulatory references to standardize clinical and compliance workflows. Its pharmacy-agnostic sourcing guidance can also help clinics standardize internal review criteria.
Key Takeaways for Safer Prescribing
The working standard is straightforward: verify, document, monitor, and stop when the trail breaks. Counterfeit or poorly documented peptides can lead to contamination, dosing errors, and hidden excipient risk. They can also create serious legal exposure when source and lot records are incomplete.
The main safeguards are clear: verify the source before first use, document lot details, review sterility and endotoxin data, give written patient instructions, and stop use when documentation is incomplete.
FAQs
How can I verify a peptide source before first use?
Confirm the active pharmaceutical ingredient is pharmaceutical-grade and comes from an FDA-registered facility. Steer clear of products labeled for research use. Those products are not cleared for human clinical use.
Before you place an order, check the pharmacy’s state license through NABP or the FDA database. Ask for a COA that covers potency and sterility. It also helps to review the facility’s inspection history and confirm compliance with USP 797/800.
What records should I keep for each peptide lot?
Keep detailed records for every peptide lot used in your practice. It helps support regulatory compliance and, just as important, patient safety.
Your documentation should include the source pharmacy, lot number, beyond-use date, clinical rationale, informed consent about its compounded nature, and any patient responses or adverse events.
That way, you have a complete audit trail for clinical quality and regulatory standards. If a question comes up later, you’re not piecing things together from memory - you have the full story in the chart.
When should I stop treatment after a suspected bad vial?
Stop treatment immediately if you think a vial may be compromised. Throw it away if the solution looks cloudy, yellow, or has visible particles.
Also stop treatment if the patient has severe or prolonged side effects. Document any adverse events and the actions taken, follow the discontinuation criteria set at therapy initiation, and tell patients to report concerns right away for clinical evaluation.