A sterile peptide can still be unsafe if endotoxin is present. That’s the main point I’d want any prescriber to remember.
If I were reviewing a compounded injectable, I’d check three things first:
- Who made it: a 503A pharmacy or a 503B outsourcing facility
- What the batch records show: not just “pass,” but the actual endotoxin number
- Which rules apply: USP <85>, USP <797>, FDA rules, and the pharmacy’s state board rules
The article’s bottom line is simple: sterility alone is not enough. Endotoxins can stay behind even after filtration or heat sterilization, and they can cause fever, chills, low blood pressure, and severe systemic reactions. For most parenteral products, the article points to the 5 EU/kg/hr limit under USP <85>, with a lower limit for intrathecal use.
Here’s the short version:
- USP <85> sets the endotoxin test framework and dose-based limit
- USP <797> sets sterile compounding rules, including endotoxin testing for high-risk CSPs made from nonsterile ingredients
- FDA oversight adds batch testing and cGMP expectations for 503B facilities
- State boards can make USP standards enforceable law for 503A pharmacies
- A COA should show numeric endotoxin results like EU/mg or EU/vial, not only pass/fail
- If multiple compounded injectables are used in one procedure, total endotoxin exposure may need to stay under the same 5 EU/kg/hr ceiling
A quick side-by-side helps:
| Topic | What I’d look for |
|---|---|
| Pharmacy type | 503A vs. 503B |
| Endotoxin proof | Numeric batch result on the COA |
| Sterility proof | Batch-linked sterility test record, when required |
| Compounding rules | USP <797> version used by that state |
| Dose safety | Whether the reported endotoxin level fits the planned dose |
So if I had to sum up the full article in one sentence, it would be this: before prescribing or stocking a compounded peptide injectable, I’d verify the pharmacy’s status, confirm batch-specific endotoxin data, and make sure the product fits both federal and state rules.
503A vs 503B vs USP Standards: Endotoxin Testing Rules for Compounded Peptide Injectables
Endotoxin Testing
sbb-itb-7164bd9
Federal framework: USP and FDA rules that set endotoxin expectations
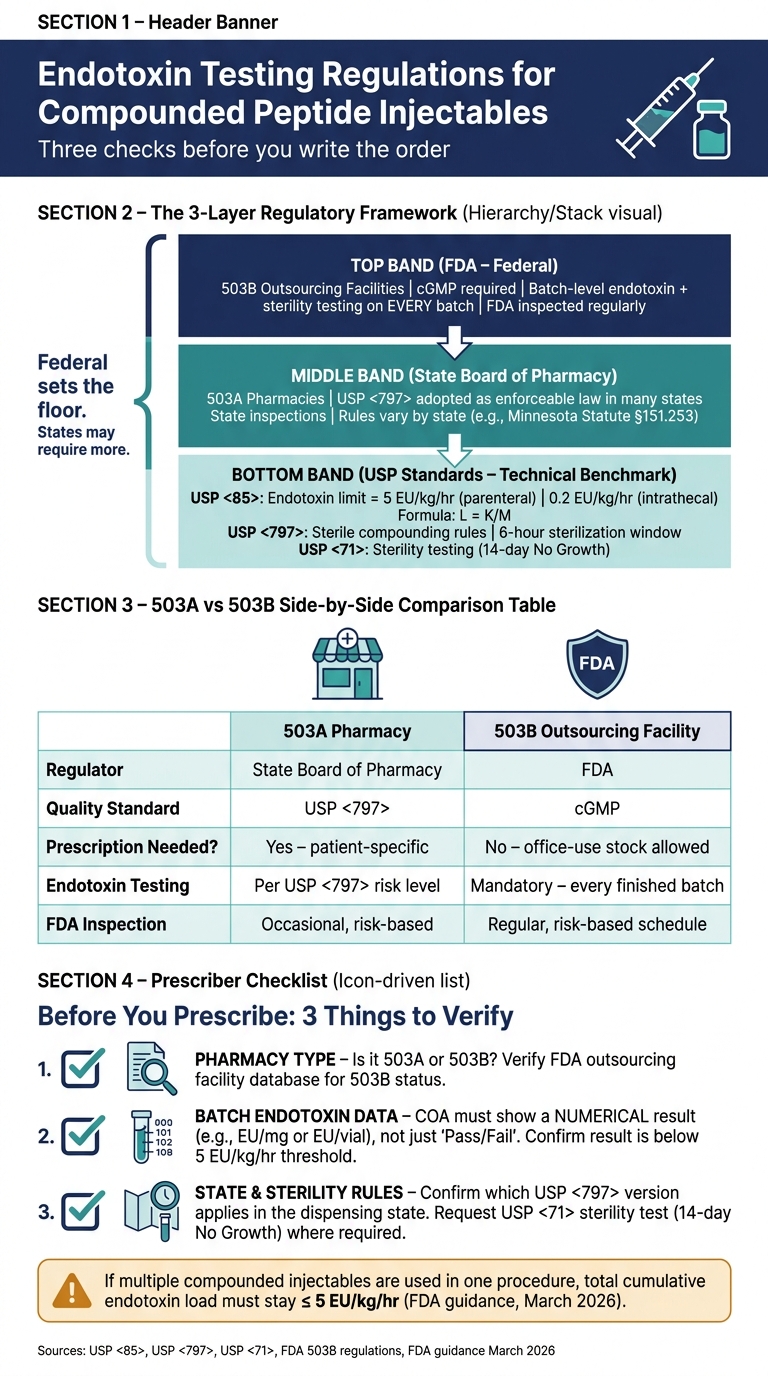
Three standards work together to define what’s acceptable for endotoxin levels in compounded sterile peptides: USP <85>, USP <797>, and FDA oversight of compounding facilities. Each one covers a different part of the picture. USP <85> deals with the test method, USP <797> covers how sterile products are compounded, and the FDA handles federal enforcement. Put them together, and they shape the records prescribers should look at before using a product.
USP <85> endotoxin limits and the K/M formula
USP <85> is the testing standard behind endotoxin safety calculations. It uses the formula L = K/M, where K = 5 EU/kg for nonintrathecal parenteral products and M is the maximum dose per kg per hour.
For intrathecal products, the limit is 0.2 EU/kg/hr.
That’s why prescribers shouldn’t stop at a simple Pass on a certificate. They should check the actual endotoxin result, such as EU/mg or EU/vial. A pass/fail label doesn’t say much on its own, especially if the compounding process behind it is weak.
USP <797> requirements for sterile compounded preparations
USP <797> covers how compounded sterile preparations, or CSPs, are made, not just how they’re tested. The revised version, effective November 2023, includes controls that have a direct effect on endotoxin risk in peptide compounding.
USP <797> is meant to prevent microbial contamination, endotoxin exposure, and compounding errors.
One rule matters a lot in day-to-day practice: the 6-hour sterilization window. Any water-containing preparation exposed to nonsterile conditions during compounding must be sterilized within 6 hours.
Preparations made from nonsterile ingredients are classified as high-risk. For those CSPs, USP <797> requires bacterial endotoxin testing. And if sterility testing has not been completed, beyond-use dates for high-risk preparations can be as short as 24 hours at controlled room temperature.
FDA expectations for compounded and investigational parenteral products
The FDA adds a federal enforcement layer on top of the USP standards. 503B outsourcing facilities must follow current Good Manufacturing Practice, or cGMP, and they can be inspected directly by the FDA. For these 503B facilities, each batch requires endotoxin and sterility testing.
FDA guidance updated in March 2026 also speaks to cumulative endotoxin exposure. If multiple compounded injectables are used in one procedure, the combined endotoxin load from all sources must stay at or below the 5 EU/kg/hr threshold.
Here’s the short version of how these standards differ and why that matters when a prescriber reviews documentation:
| Standard | Scope | Key Requirement | Prescriber Relevance |
|---|---|---|---|
| USP <85> | Analytical method | Defines the K/M formula and the 5 EU/kg limit | Verify quantitative values on COAs |
| USP <797> | Sterile compounding practices | Mandates testing for CSPs made from nonsterile ingredients and includes a 6-hour sterilization rule | Confirm the pharmacy has process controls in place |
| FDA (503B/Guidance) | Federal regulatory oversight | Requires batch-level testing and cumulative exposure review | Confirm batch-level evidence and total procedural endotoxin load |
These federal standards set the floor. State boards may ask for more.
State regulation: How boards of pharmacy apply endotoxin testing rules
Federal standards set the floor. State boards decide how those rules play out for 503A pharmacies. In many states, USP standards are adopted by reference, which turns them into enforceable pharmacy law for 503A compounding. For prescribers, the main issue is simple: which state rule applies to the pharmacy supplying the injectable?
How state adoption of USP <797> affects sterile peptide compounding
When a state board formally adopts USP <797>, compliance becomes a legal requirement, not just a best practice. That gives state boards room to inspect facilities, review staff training, and cite gaps in compliance without waiting for FDA action.
State examples and stricter local requirements
Minnesota is a clear example of how state adoption turns USP <797> into enforceable compounding law. Minnesota Rule 6800.3300, subpart 2, and Minnesota Statute § 151.253 require licensed pharmacies that compound sterile products to follow USP <797> standards. Minnesota also requires sterile compounding to meet USP <797>.
States are also putting more weight on independent verification instead of relying only on supplier-provided paperwork. That matters in practice. Prescribers should ask for lot-specific endotoxin and sterility testing results when reviewing a pharmacy.
What varies across states and why prescribers should verify local rules
Not every state has adopted the November 2023 revision of USP <797>. Some still enforce earlier versions. That can change rules for beyond-use dating, environmental monitoring frequency, and high-risk CSP testing from one state to another. Inspection priorities also differ by state, which affects the records pharmacies need to keep.
The practical point is straightforward: a pharmacy that meets the rules in one state may fall short in another. If you work across state lines, or use a pharmacy licensed in a different state from where you practice, check which version of USP <797> applies and whether extra local rules are in force.
| Regulatory Layer | What It Governs | Example Endotoxin-Related Requirement | Why It Matters for Prescribers |
|---|---|---|---|
| Federal (FDA) | 503B outsourcing facilities & bulk ingredients | cGMP compliance; batch-level endotoxin and sterility testing | Helps confirm large-scale batch quality and ingredient legality |
| State Board of Pharmacy | 503A pharmacies | Mandatory adherence to USP <797> and USP <85> for sterile injectables | Sets the local legal standard and supports state inspections and citations |
| USP Standards | Clinical and lab benchmarks | USP <85> endotoxin limits; sterile compounding rules in USP <797> | Serves as the technical benchmark used by state and federal inspectors |
Federal compliance does not guarantee state compliance. Prescribers should verify the pharmacy's state licensure and the USP <797> version it follows. That check points to the records prescribers should review before using the product.
What prescribers should review before using compounded peptide injectables
Before you prescribe or stock a compounded peptide injectable, check two things first: the pharmacy type and the batch records. That gives you a simple, practical checklist to work from instead of guessing your way through it.
503A versus 503B: Why the distinction changes prescriber oversight
The pharmacy type changes what records you should ask for before use.
A 503A pharmacy needs a patient-specific prescription for each dispense. Testing frequency follows USP <797> risk levels and any state rules that apply. A 503B outsourcing facility can supply office-use stock without a patient-specific prescription and must perform endotoxin and sterility testing on every finished batch. If you're buying from a 503B, ask for batch-specific endotoxin and sterility results before ordering.
| Feature | 503A Pharmacy | 503B Outsourcing Facility |
|---|---|---|
| Primary Regulator | State Board of Pharmacy | FDA |
| Quality Standard | USP <797> | cGMP |
| Prescription Requirement | Patient-specific required | Office-use permitted without patient-specific prescription |
| Endotoxin Testing | Per USP <797>, often lot-based | Mandatory for every finished batch |
| FDA Inspection | Occasional, risk-based | Regular, risk-based schedule |
You can verify 503B status in the FDA's outsourcing facility database. It's also smart to check for recent warning letters before you place an order. That one classification shapes the level of oversight you should apply and the records you should request.
What documentation to request and how to read it
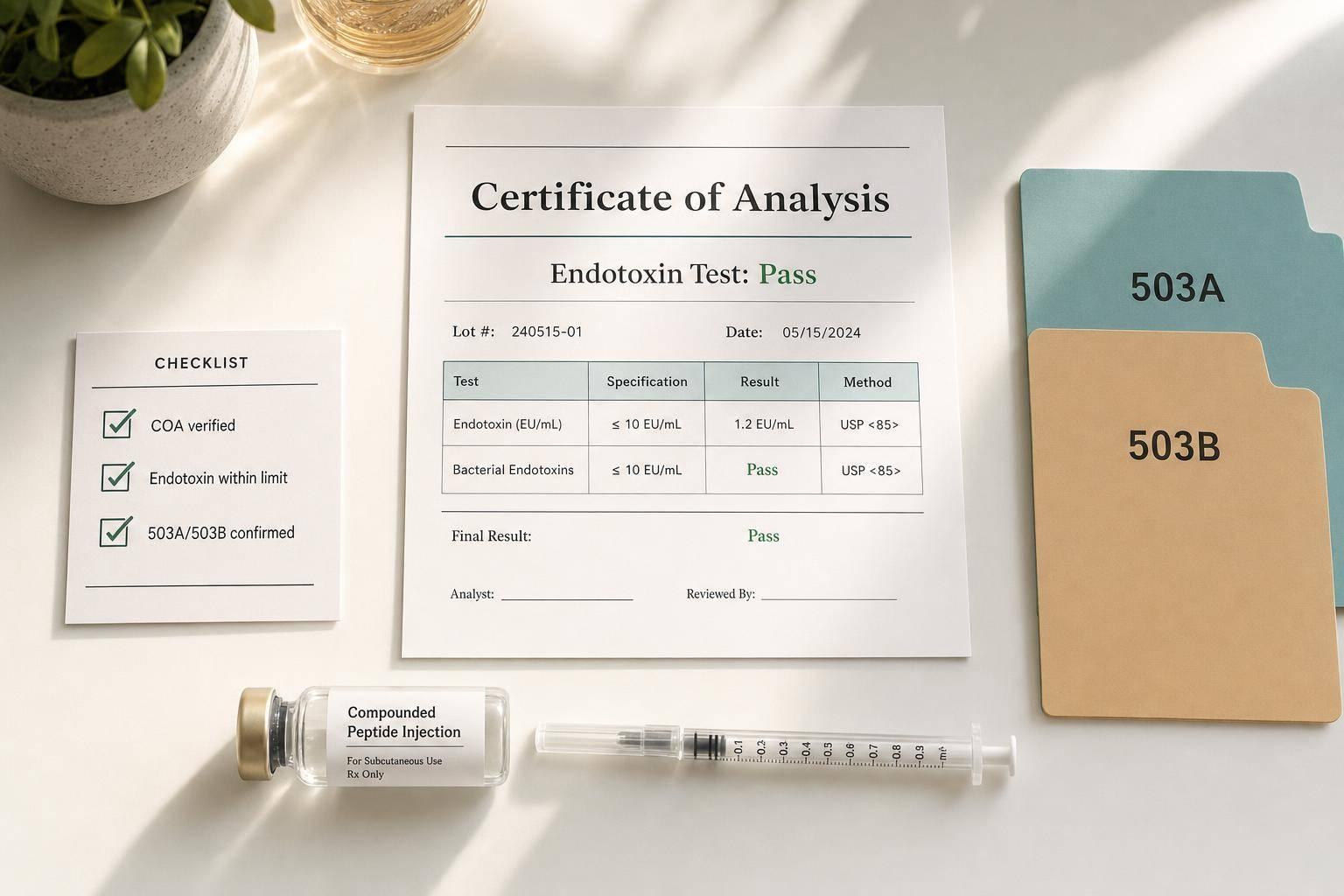
A Certificate of Analysis, or COA, is the first document to request. But here's the catch: not every COA tells you enough.
Ask for a COA that includes:
- Identity confirmation by mass spectrometry
- Purity data by HPLC
- Batch-specific endotoxin results from an LAL or rFC assay
Don't settle for a simple pass/fail line. You need the numerical endotoxin result - for example, EU/mg - so you can judge the actual dose exposure.
Use that value to check dose-level exposure against the 5 EU/kg/hr threshold for parenteral routes. Then review the basics that are easy to miss but matter a lot: the COA date, lot number, and whether the test results are tied to that exact batch. If the product comes in a multi-dose vial, review the stability data too. And where required, make sure sterility testing under USP <71> is included.
That set of records is what you should review before prescribing, stocking, or compounding.
How PeptidePrescriber can support regulatory review and clinical decision-making
Sorting through the regulatory landscape of compounded peptides while running a clinic can eat up a lot of time. PeptidePrescriber brings together the regulatory references, evidence-based peptide monographs, and clinical tools prescribers use to review documentation and make defensible sourcing decisions, with pharmacy-agnostic sourcing guidance.
The table below lines up common prescriber decision points with the rule involved, what to check, and what acceptable proof looks like.
| Prescriber Decision Point | Relevant Regulation | What to Verify | Acceptable Evidence |
|---|---|---|---|
| Sourcing for office stock | Section 503B | FDA registration status | Valid FDA 503B outsourcing facility listing |
| Patient-specific order | Section 503A | State pharmacy license | Active state license in the prescriber's state |
| Pyrogen safety | USP <85> / <86> | Endotoxin concentration | Numerical EU/mg result on COA |
| Sterility assurance | USP <71> | Sterility testing | 14-day incubation "No Growth" report |
For prescribers starting or growing a peptide practice, having these references in one place can cut down the time spent tracking documents and help support the clinical record if questions come up later.
Conclusion: Key endotoxin testing points for prescribers
Core takeaways for clinical practice
For prescribers, this comes down to three checks before you write the order. Endotoxin control is a patient-safety issue, not a paperwork issue.
USP <85> sets the endotoxin limit at < 5 EU/kg for most parenteral products. Check the COA and make sure it shows a numerical endotoxin result, not just a simple pass/fail note.
State rules can go beyond the federal baseline, so the pharmacy's type matters. It tells you how much oversight sits behind the product.
- 503B outsourcing facilities are subject to FDA cGMP requirements and must test every batch.
- 503A pharmacies are mainly regulated by states and follow USP <797> plus state board rules, which can differ.
That means prescribers should confirm the rules that apply in the dispensing state.
Before ordering, review the pharmacy's registration status, batch-specific endotoxin data, and required sterility results.
FAQs
How do I calculate endotoxin exposure from a planned dose?
Compare the planned dose to the USP <85> safety limit of 5 EU/kg/hour.
If the patient’s weight is in pounds, convert it to kilograms first using 1 lb ≈ 0.45 kg. Then multiply the weight in kilograms by 5 to find the maximum tolerable endotoxin dose per hour.
For example, a 176 lb (80 kg) patient has a limit of 400 EU/hour.
If the planned dose goes above that limit, the risk of a pyrogenic response goes up, including fever or sepsis.
What should I do if a COA only shows pass/fail?
A COA that only shows pass/fail isn't enough to check clinical safety. For injectable peptides, it should show the measured endotoxin level in EU and confirm that it is below 5 EU/mL.
If that number is missing, ask the pharmacy for a detailed report. You can also get independent third-party lab testing so you have precise, verifiable results.
Which state’s USP <797> rules apply to my order?
The USP <797> rules that apply usually depend on the state where the compounding pharmacy is located.
Most states use the federal USP <797> standard as their baseline. But some states go further and add stricter rules for testing, recordkeeping, and beyond-use dating.
That’s why it’s worth checking which state’s rules apply to the pharmacy filling your order. A pharmacy in one state may follow a different set of requirements than a pharmacy in another, even when both are working from USP <797>.