
If you want the short answer: soy peptides have the best human data, while marine, algae, and animal-protein peptides look stronger in lab and animal work than in clinical use so far.
I’d sum up the article like this: these four peptide groups can affect blood lipids and liver fat through a few main mechanisms of action - slowing cholesterol production, increasing LDL clearance, binding bile acids, and reducing fat absorption in the gut. But the gap between lab results and human results is still the main issue.
Here’s what matters most:
- Soy-derived peptides: best studied in people; usually linked with modest drops in LDL-C and total cholesterol
- Marine peptides: strongest signal for triglycerides and hepatic fat, mostly from animal studies
- Algae-derived peptides: broad effects on TC, TG, LDL-C, and liver fat, but human peptide data are still sparse
- Animal-protein hydrolysates: mixed but strong preclinical lipid effects; limited human trials
- Main limit across all four: oral delivery, digestion before absorption, and product standardization
A few numbers stand out right away:
- 25 g/day of soy protein for 6 weeks lowered LDL-C by 4.76 mg/dL and TC by 6.41 mg/dL
- In mice, Manila clam peptides cut hepatic lipid droplets by 74.12%
- Spirulina hydrolysate showed 66.23% pancreatic lipase inhibition
- Freshwater clam hydrolysate cut plasma triglycerides by 65% in preclinical work
Bioactive Peptides from Fermented Plant-based Foods: Current trends and Challenges
sbb-itb-7164bd9
Quick Comparison
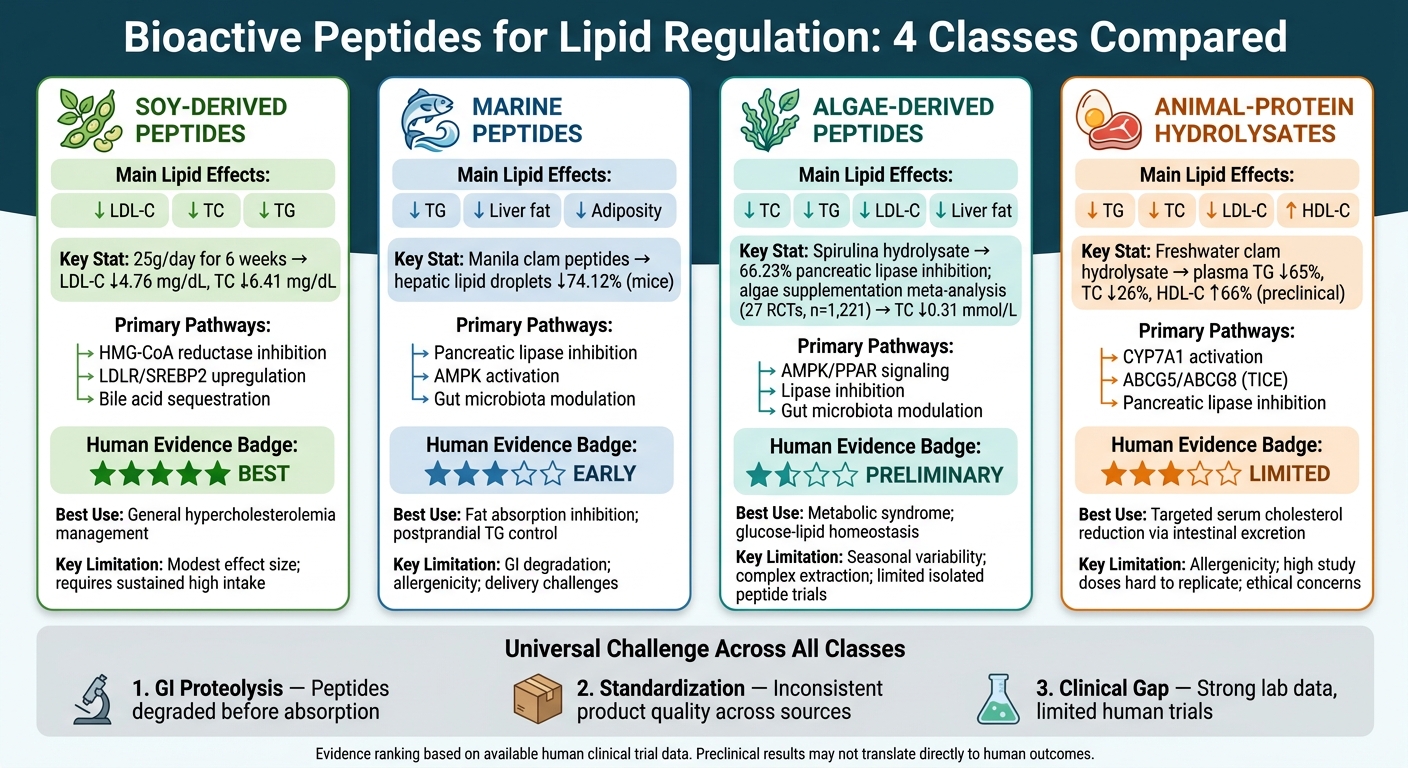
Bioactive Peptides for Lipid Regulation: 4 Classes Compared
| Peptide Class | Main Lipid Pattern | Main Pathways | Human Evidence |
|---|---|---|---|
| Soy-derived | ↓ LDL-C, ↓ TC, ↓ TG | HMG-CoA reductase inhibition, LDLR/SREBP2, bile acid effects | Best among the four |
| Marine | ↓ TG, ↓ liver fat, ↓ adiposity | Pancreatic lipase inhibition, AMPK, HMGCR, gut microbiota shifts | Early but limited |
| Algae-derived | ↓ TC, ↓ TG, ↓ LDL-C, ↓ liver fat | AMPK, PPAR signaling, lipase inhibition | Mostly supplementation, not isolated peptides |
| Animal-protein hydrolysates | ↓ TG, ↓ TC, ↓ LDL-C, some ↑ HDL-C | CYP7A1, ABCG5/ABCG8, intestinal cholesterol excretion | Limited |
Bottom line: if I were ranking these by current clinical support, I’d put soy first. If I were ranking them by how strong the preclinical lipid effects look, marine and some animal-protein peptides would be close contenders. The rest of the article breaks down where each class looks strongest - and where the data still fall short.
1. Soy-Derived Peptides
Soy is the most studied dietary protein source for lipid management, so it serves as the benchmark for plant-derived peptides. Its two main protein fractions - β-conglycinin (7S) and glycinin (11S) - produce bioactive peptides linked to lower LDL-C, TC, TG, and hepatic lipid accumulation. That makes soy the main reference point when comparing peptides from marine, algae-derived, and animal-protein sources.
Lipid Outcomes
In people, the lipid-lowering effect is measurable, but modest. A meta-analysis of 43 controlled clinical trials found that taking 25 g of soy protein daily for 6 weeks lowered plasma LDL-C by 4.76 mg/dL and TC by 6.41 mg/dL. Not huge numbers, but not nothing either.
One peptide that helps show how soy works is the dipeptide Ser-Tyr (SY). It has been linked to lower TG synthesis and reduced ApoB secretion.
Target Pathways
Soy peptides seem to work through two main routes: they slow lipid synthesis and help the body clear cholesterol.
On the synthesis side, soy peptides suppress cholesterol production by inhibiting HMGCR directly. For example, IAVPGEVA inhibits HMGCR activity by up to 75% in vitro. Soy peptides also activate AMPK, which then inactivates HMGCR.
They also affect cholesterol uptake and transport. Peptides such as YVVNPDNDEN increase mature SREBP-2 levels, which boosts LDL receptor (LDLR) expression. Another peptide, FVVNATSN, increases LDLR transcription in hepatocytes by 248.8% compared with untreated controls.
On top of that, soy peptides may help the body get rid of cholesterol. They upregulate ABCG5 and ABCG8 in the small intestine and can sequester bile acids, which helps block their reabsorption.
Translational Limits
There’s a catch. In humans, LDL-C reduction is usually modest - around 3% to 5% - and it depends on sustained high intake. Bioavailability, stability, and long-term safety are still limiting issues. Clinicians must also apply rigorous patient selection criteria to ensure these interventions are appropriate for the individual's metabolic profile. Large-scale production is also slow and constrained by stability problems.
So, soy proteins fit best in the functional food category: useful in practice, but modest in effect.
2. Marine Peptides
Marine peptides from cod, abalone, monkfish, clams, tuna, squid, and salmon work through a few main routes: they can inhibit pancreatic lipase, inhibit HMGCR, activate AMPK, and in some cases shift the gut microbiota. Put simply, they seem to hit lipid metabolism from two sides. They can reduce how much fat gets absorbed in the gut, and they can cut down how much fat builds up in the liver.
That pattern shows up most clearly in lower TG exposure and less hepatic fat storage.
Lipid Outcomes
In HFD-fed mice, Manila clam peptides at 600 mg/kg reduced hepatic lipid droplets by 74.12%. They also cut epididymal fat by 71.32% and perirenal fat by 70.53%. Those are large drops, and they line up with the idea that these peptides affect both fat handling and fat storage.
Some marine peptides also act earlier in the digestion process. Abalone peptides such as QDAVMPNPF and SPADIGFH reduced cholesterol micelle solubility by 47.94% and 45.23%. Cod peptides GSPPPSG and KLEGDLK inhibited pancreatic lipase. Taken together, the clearest lipid signals across models are lower TG and lower hepatic lipid load. There is less direct evidence for ApoB and AI.
These findings suggest two linked effects: blocking part of lipid absorption upstream and slowing hepatic lipogenesis downstream.
Target Pathways
Mechanistically, marine peptides differ from soy peptides because they act more directly on fat digestion and fatty acid use. AMPK activation suppresses SREBP-1c and increases PPARα and CPT-1, which shifts metabolism toward fatty acid oxidation. In plain terms, the liver is pushed away from making fat and toward burning it.
Abalone peptides add another angle. Peptides such as APDMAFPR act as competitive HMGCR inhibitors, with inhibition rates of 51.8%–59.5% in vitro. That was comparable to atorvastatin at 0.5 mM. Clam-derived peptides may also affect metabolism through the gut. They increased Bacteroidetes and Alistipes while decreasing Firmicutes.
Evidence Level
Most of the evidence is still preclinical. That said, there is an early human signal. A 12-week double-blind RCT in prediabetic patients found that oyster peptides improved TC, LDL-C, and TG. So the case for marine peptides is not just from animal work, but clinical data are still limited. Clinicians can follow clinical insights for updates on emerging human trials.
Translational Limits
The biggest hurdle is bioavailability. Marine peptides are water-soluble, which can reduce membrane permeability, and gastric proteases may degrade them before they are absorbed. That makes delivery a big deal, requiring practical guides for proper administration, not a side issue.
One workaround is nano-liposomal encapsulation. At about 157 nm, this approach improved stability, transport, and encapsulation efficiency, reaching 61.2% ± 3.2%. Even so, dose standardization remains hard because many structure-function relationships have not yet been mapped clearly.
This benchmark sets up the next comparison with algae-derived peptides.
3. Algae-Derived Peptides
Peptides from Chlorella pyrenoidosa and Spirulina platensis have been linked with lower TC, TG, LDL-C, and less fat buildup in the liver. Their effects on HDL-C are less consistent.
Lipid Outcomes
One of the clearest cases is peptide T1 (SISISVAGGGR) from Chlorella pyrenoidosa. In HFD-fed mice, doses of 100–300 mg/kg/day lowered serum TC, TG, and LDL-C, increased HDL-C, and reduced hepatic lipid accumulation and chronic inflammation. T1 also stayed stable after simulated gastric and intestinal digestion. That matters because it suggests the peptide may keep working after passing through the digestive tract.
Spirulina platensis hydrolysates show a somewhat different pattern. Along with lowering serum TC, they have also been tied to weight reduction, likely through central lipid signaling.
Target Pathways
Algal peptides seem to work through several routes at once, including AMPK, PPAR-α/γ signaling, lipase inhibition, and gut microbiota modulation. In plain terms, they may affect how the body handles fat, how much fat gets absorbed, and how inflammation interacts with lipid balance.
There are also direct enzyme effects. Spirulina platensis protamex hydrolysate showed a pancreatic lipase inhibition rate of 66.23%. Chlorella pyrenoidosa alcalase hydrolysates showed an inhibitory IC50 of 87.79 µg/mL. T1 may also have a prebiotic-like role, helping maintain gut microbial stability and lowering systemic inflammation tied to lipid dysregulation.
Evidence Level
The strongest data so far come from lab and rodent studies. Human evidence mostly comes from algae supplementation rather than isolated peptides, which is an important distinction.
A meta-analysis of 27 RCTs with 1,221 participants found that algae supplementation lowered TC by an average of 0.31 mmol/L. Effects on LDL-C and TG were mixed, and longer human trials are still needed. So while algae peptides look promising, they are not as far along clinically as animal-protein hydrolysates.
Translational Limits
There are a few practical problems here. Protein content in macroalgae shifts with season, growing conditions, and geography, which makes standardization hard. Enzymatic hydrolysis is specific, but it is also costly and time-consuming. On top of that, large-scale production that keeps peptide stability intact is still an open issue.
Oral bioavailability is another gap. Most algal peptides still do not have clear bioavailability data, even though T1 showed digestive stability in simulation studies.
4. Animal-Protein Hydrolysate Peptides
Animal-protein hydrolysates show a broad mix of effects on blood lipids and liver fat in this comparison. The best-studied sources here include fish, egg white, casein, collagen, and bovine heart. Across those sources, researchers have reported changes in plasma lipids as well as hepatic fat.
Lipid Outcomes
The lipid results vary by source, but some of the numbers are striking. In plasma, freshwater clam hydrolysate at 16% of the diet cut plasma triglycerides by 65%, lowered total cholesterol by 26%, and increased HDL-C by 66%. Sardinelle hydrolysates reduced serum triglycerides by up to 46% and LDL-C by 40%. Egg white hydrolysates also showed an effect, reducing plasma triglycerides by 28% and total cholesterol by 13% over 20 weeks in rats.
Liver lipid data point in the same direction. Chicken collagen hydrolysate at 10% of the diet lowered hepatic triglycerides by 42% and hepatic total cholesterol by 24% in atherosclerosis-prone mice. The cattle heart dipeptide Phe-Pro also lowered total cholesterol and non-HDL-C, while increasing HDL-C and fecal acid steroid excretion.
Taken together, these findings suggest action at two main sites: the gut, where cholesterol handling can shift, and the liver, where lipid synthesis and storage can change.
Target Pathways
This group does not act through a single pathway. Instead, different peptides seem to hit different parts of lipid metabolism.
Casein-derived peptides, SQSKVLPVPQK and HPHPHLSF, promote trans-intestinal cholesterol excretion through ABCG5/ABCG8, which increases fecal cholesterol secretion. Whey-derived lactostatin (IIAEK) activates CYP7A1 through calcium signaling. Chicken collagen appears to suppress FAS and modulate PGC-1α, which helps reduce hepatic lipid buildup.
That range of mechanisms helps explain why results are mixed from one source to another and from one model to the next. Fish peptides are not doing the exact same job as casein peptides, and that matters.
Evidence Level
Human evidence exists, but it is still limited. For practitioners, clinical resources for peptide-prescribing professionals can help bridge the gap between research and practice. A 3-month trial published in Food & Function in 2013 found that marine collagen peptides significantly reduced plasma triglycerides, total cholesterol, LDL-C, and free fatty acids while increasing HDL-C in subjects with type 2 diabetes.
Even so, most of the evidence still comes from in vitro work and animal models, including ApoE-null mice and Zucker rats. So while the signal is promising, the data base is still tilted toward preclinical research.
Translational Limits
Dose is one obvious problem. Many studies use 0.5-1.0 g/kg, which is hard to match in day-to-day intake. On top of that, gastric pepsin and brush-border peptidases can break down bioactive sequences before they are absorbed.
Smaller dipeptides such as Phe-Pro may have an edge here because they can be absorbed through hPepT1/2 transporters. There is also a manufacturing issue: the choice of hydrolysis protease strongly changes peptide yield, which makes product consistency hard to control.
Mechanisms, Evidence, and Clinical Relevance
Across peptide classes, the pattern is pretty clear: plant peptides usually act on cholesterol synthesis, while marine peptides and some animal peptides more often act on fat absorption. That split matters because it shapes where each class makes the most sense in clinical practice.
Bile acid handling is another point of separation. Some peptides bind bile acids directly, while others increase bile acid synthesis. For example, soy peptide IAVPGEVA binds cholic and deoxycholic acid in the GI tract. By contrast, milk-derived lactostatin (IIAEK) activates CYP7A1 through calcium signaling, which increases hepatic bile acid conversion.
Food-derived peptides may also affect PCSK9. One study in Trends in Food Science & Technology found that Alcalase-digested hempseed lowered PCSK9 protein levels in HepG2 cells, while pepsin-digested hempseed increased PCSK9 expression.
Human trials are still the main bottleneck for clinical use.
The practical issue isn’t whether these peptides can affect lipid metabolism. It’s which class has the best match between mechanism and evidence. The table below compares pathway focus, lipid effects, evidence level, and clinical use.
| Peptide Class | Primary Pathway Emphasis | Key Lipid Endpoints | Clinical Applicability |
|---|---|---|---|
| Soy-Derived | HMGCoAR inhibition; SREBP2/LDLR activation; TICE (ABCG5/8) | ↓ LDL-C, ↓ TC, ↓ TG | High - best clinical trial support |
| Marine | Pancreatic lipase inhibition; NPC1L1 downregulation; PPAR-γ/C/EBPα | ↓ TG, ↓ TC, ↓ Adiposity | Moderate - human data limited |
| Algae-Derived | HMGCoAR inhibition; AMPK/MAPK signaling; PPAR-α | ↓ TC, ↓ TG, ↓ Liver fat | Preliminary - clinical trials needed |
| Animal-Protein Hydrolysates | CYP7A1 activation (milk); TICE/ABCG5 (casein); Pancreatic lipase inhibition (collagen) | ↓ TC, ↓ LDL-C, ↑ Bile acid excretion | Moderate - limited human data |
Soy-derived peptides have the strongest human evidence. The other classes are still mostly preclinical. So while the end target often overlaps, the bigger differences show up in how they work and how much human data backs them up.
Pros and Cons of Each Peptide Class
Not all peptide classes work the same way. Some look stronger in lab settings. Others have better human data. And some sound promising on paper but run into problems once you get to sourcing, digestion, or day-to-day use.
This is the main tradeoff: potency, delivery, and clinical fit don’t always line up.
Soy-derived peptides have the strongest clinical evidence base, which gives them an edge for general hypercholesterolemia management. But there’s a catch. Source variability and the need for precise hydrolysis can make product-to-product consistency harder to control.
Marine peptides show the strongest in vitro potency. That sounds great at first glance, but lab potency alone doesn’t guarantee oral efficacy. GI degradation, delivery needs, and allergenicity are still the big obstacles for oral use.
Algae-derived peptides stand out for their broad multi-pathway effects. That makes them interesting for metabolic syndrome and glucose-lipid homeostasis. Still, extraction can be hard, contamination risk is a real issue, and clinical data remains limited.
Animal-protein hydrolysates offer useful intestinal cholesterol effects, including targeted serum cholesterol reduction through intestinal excretion. They also show high bioavailability. The downside is pretty clear: allergenicity, cost, and ethical concerns can narrow their use across different patient groups.
| Peptide Class | Key Advantages | Main Limitations | Best-Supported Use Context |
|---|---|---|---|
| Soy-Derived | Strongest clinical evidence base | High source variability; requires precise hydrolysis | General hypercholesterolemia management |
| Marine | Strongest in vitro potency | GI instability; allergenicity; delivery requirements | Fat absorption inhibition; postprandial triglyceride control |
| Algae-Derived | Broad multi-pathway effects | Complex extraction; contamination risk; limited clinical trials | Metabolic syndrome; glucose-lipid homeostasis |
| Animal-Protein | Targeted intestinal cholesterol excretion; high bioavailability | Allergenicity; ethical and cost concerns | Targeted serum cholesterol reduction via intestinal excretion |
Conclusion
Of the four peptide classes covered here, soy-derived peptides have the strongest human data for lowering lipids. That lead seems to come mainly from HMG-CoA reductase inhibition and LDLR upregulation.
Outside soy, the picture changes. Marine and algae-derived peptides still look promising for triglyceride control and fatty acid oxidation, but the human evidence is thin so far. Animal-protein hydrolysates show much the same split: strong preclinical results, but only limited clinical confirmation.
Across all peptide classes, one issue keeps getting in the way: delivery. Low oral bioavailability, gastrointestinal proteolysis, and uneven standardization still slow translation from lab findings to patient use. Because of that, clinical adoption is still premature.
For now, bioactive peptides make more sense as adjunct nutraceuticals than as substitutes for established lipid-lowering therapy. In this comparison, the ranking comes down to clinical proof, not just mechanistic plausibility.
FAQs
How do bioactive peptides actually lower cholesterol and triglycerides?
Bioactive peptides can help regulate lipids in two main ways: through what happens in the diet and through what happens inside the body.
In the gut, these peptides may lower dietary cholesterol absorption by binding bile acids and reducing cholesterol micellar solubility. Put simply, they can make it harder for cholesterol to get absorbed during digestion.
After absorption, they may also help on the metabolic side. Some peptides appear to reduce cholesterol production, promote fatty acid oxidation, and influence genes such as SREBP2, LDLR, and PCSK9 in ways that improve LDL uptake.
Why do soy peptides have stronger human evidence than marine, algae, or animal peptides?
Soy peptides have stronger human evidence for one main reason: soy protein has been studied for a long time as a functional food.
A big turning point came in 1999, when the U.S. Food and Drug Administration approved a health claim linking soy protein to a lower risk of cardiovascular disease. That decision helped spark more research.
Soy is also a major protein source with a favorable amino acid balance. Because of that, researchers have used it often in large clinical and dietary studies focused on cholesterol and hyperlipidemia.
Can bioactive peptides replace statins or other lipid-lowering medications?
No. Bioactive peptides are not considered replacements for statins or other prescribed lipid-lowering drugs at this point.
Research suggests they may help modulate lipid metabolism. But right now, they’re mostly being studied as nutraceutical candidates, not as stand-ins for standard prescription treatment.
Their use in clinical settings is still limited by a few major hurdles, including oral bioavailability and the need for more human studies.