
Brown fat can help burn extra energy, but it is not a stand-alone answer for obesity. From the article, I’d sum it up this way: peptide-linked pathways may support heat production through 4 main routes - UCP1 signaling, mitochondrial heat production, adipocyte browning, and endocrine crosstalk - but the human effect looks modest, and the strongest clinical use today is still with GLP-1 drugs for appetite and blood sugar control, not proven brown-fat targeting.
If you want the short version, here it is:
- Brown adipose tissue (BAT) burns fuel to make heat.
- Beige fat is white fat that starts acting more like brown fat.
- Full BAT activation may add about 170 kcal/day and about 2%–5% of resting metabolic rate.
- People with detectable BAT often have lower fasting glucose, lower A1C, lower triglycerides, and smaller waist size.
- Human cold-exposure studies showed insulin sensitivity gains of about 20% in healthy men and more than 40% after 10 days in people with type 2 diabetes.
- The peptide story is mixed:
- GLP-1: best clinical footing, but BAT effects are still secondary
- FGF21: tied to BAT activity and metabolic markers, still early
- Irisin: strong animal and cell data, but human data is uneven
What matters most is how each pathway works:
- UCP1 signaling = the direct heat switch
- Mitochondrial heat production = how much heat the cell can keep making
- Adipocyte browning = adding more heat-capable cells
- Endocrine crosstalk = signals between fat, liver, muscle, gut, brain, and more
Why Is Brown Fat Protective Against Metabolic Disease
sbb-itb-7164bd9
Quick Comparison
| Mechanism | What it does | Main tissue | What it may affect most | Human support |
|---|---|---|---|---|
| UCP1 signaling | Turns fuel into heat | Brown fat, beige fat | Energy expenditure | Limited direct proof |
| Mitochondrial heat production | Sets heat-making capacity | Brown fat, beige fat | Resting fuel burn | Limited |
| Adipocyte browning | Converts white fat toward beige fat | Subcutaneous white fat | Body composition over time | Early |
| Endocrine crosstalk | Links BAT with other organs | BAT, liver, muscle, brain, gut | Glucose, lipids, insulin sensitivity | Best current support |
For me, the main takeaway is simple: brown fat biology is promising, but current obesity care should still focus on body weight, A1C, triglycerides, and liver fat - not BAT alone. The article then breaks down each of these four routes in plain clinical terms.
Why Brown Fat Activation Matters in Obesity Medicine
40.3% of U.S. adults meet the criteria for obesity, and 9.7% meet the criteria for severe obesity. That’s why BAT matters in a clinical sense, not just a lab one. It can increase energy expenditure and shift how the body uses fuel, which ties it to the same markers clinicians watch at routine visits.
When BAT is fully switched on, it can add about 170 kcal/day in energy expenditure and make up roughly 2–5% of resting metabolic rate. On its own, that’s not huge. But over time, and paired with diet changes or drug treatment, it can add up.
There’s also a clear link between detectable BAT and better metabolic health. Adults with detectable BAT tend to have lower fasting glucose and A1C, even after adjusting for age, sex, and body fatness. BAT-positive adults also tend to have a smaller waist circumference and lower triglycerides. In plain terms, BAT lines up with measures clinicians already care about: glucose, A1C, triglycerides, and waist size.
Intervention data points in the same direction. Cold-induced BAT activation has been shown to improve whole-body insulin sensitivity by about 20% during euglycemic clamp testing in healthy men. And after ten days of cold acclimation, people with type 2 diabetes saw peripheral insulin sensitivity increase by over 40%. Those changes show up in glucose control, adiposity, and lipid markers.
BAT activation should be seen as a support tool, not a standalone fix. Body weight is still the main outcome. BAT is a secondary lever, not the center of obesity treatment. The next four mechanisms show the biologic routes peptides may use to boost that thermogenic response as part of standard obesity care.
1. UCP1 Signaling
Uncoupling Protein 1 (UCP1) is a mitochondrial membrane protein found in the inner mitochondrial membrane of brown and beige adipocytes. Its job is simple but powerful: it uncouples oxidative phosphorylation, so the mitochondrial proton gradient is released as heat instead of being used to make ATP.
Sympathetic stimulation turns UCP1 on. When the body is exposed to cold, it releases norepinephrine. That norepinephrine binds to β3-adrenergic receptors on brown adipocytes, increases cAMP, activates PKA, and triggers lipolysis. The free fatty acids (FFAs) produced in that process do two things: they support oxidative metabolism and remove nucleotide-mediated inhibition of UCP1, which activates the protein.
Peptides may strengthen this pathway by increasing sympathetic signaling, boosting UCP1 expression, or increasing the pool of UCP1-positive cells. That’s the core UCP1 route. But UCP1 alone isn’t the whole story. A cell also needs enough mitochondrial hardware to produce a strong thermogenic response.
UCP1-mediated thermogenesis increases energy expenditure on the “energy out” side of the equation, and it does so without requiring physical activity.
Classical BAT in supraclavicular, cervical, and paravertebral depots expresses UCP1, and subcutaneous white fat can also recruit beige adipocytes. In plain terms, thermogenic tissue isn’t fixed. It can grow.
Most peptide interventions act upstream of UCP1 rather than binding to UCP1 itself. They tend to:
- increase UCP1 gene expression
- improve adrenergic sensitivity
- expand the number of UCP1-expressing cells
That matters because UCP1 expression is only part of the equation. Actual heat output still depends on how much mitochondrial machinery the cell has to support the process.
One clinical study gives a useful example. Over 24 weeks, the share of participants with detectable BAT activity on FDG-PET/CT increased from 41.2% to 64.7% in the tirzepatide group, while the placebo group showed no change (P = .005). That pattern suggests BAT activation extended beyond appetite suppression alone and points toward the upstream peptide signals discussed next.
2. Mitochondrial Heat Production
UCP1 flips the switch, but mitochondrial capacity sets the ceiling for how much heat brown fat can keep producing. Once UCP1 turns on, mitochondria in brown adipocytes let protons leak back across the inner mitochondrial membrane. Instead of using that proton motive force to make ATP, the cell burns it off as heat. So the key issue becomes simple: how much thermogenic machinery does the cell have to keep that process going?
BAT can also make heat through a UCP1-independent creatine cycle, which adds to total heat output when UCP1 is limited.
Representative Peptide Pathways
A few peptide-linked pathways help support this heat-producing setup.
- FGF21 promotes mitochondrial biogenesis and thermogenic gene expression.
- Irisin promotes mitochondrial biogenesis and beige-fat thermogenesis.
As mitochondria expand, white fat can also start taking on brown-like traits.
Target Tissues and Organ Axis
The main targets are classical BAT and beige adipocytes recruited from white fat. As this program spreads into white fat, it starts to overlap with adipocyte browning.
Obesity-Treatment Relevance
More mitochondrial heat production can increase resting energy expenditure and lipid oxidation. In plain terms, the body burns more fuel at rest, which may help support weight loss and metabolic improvement when paired with diet, lifestyle changes, or pharmacotherapy.
That said, human evidence is still limited, so this mechanism makes the most sense as a supporting piece rather than a standalone fix.
3. Adipocyte Browning
Unlike UCP1 signaling and mitochondrial heat production, browning increases the number of cells that can burn energy as heat. White adipocytes can shift into beige adipocytes, picking up thermogenic genes, more mitochondria, and inducible UCP1. In plain English, white fat starts acting a bit more like heat-making fat.
Primary Thermogenic Pathway
PGC-1α is a main driver here. It pushes mitochondrial biogenesis and turns on thermogenic gene expression. Cold exposure, β-adrenergic input, and peptide signals can trigger a cAMP–PKA–p38 MAPK–PGC-1α cascade, which increases UCP1 and fatty acid oxidation.
Beige adipocytes don’t do much at baseline. Their UCP1 activity stays low until the right signal shows up. But when it does, they can ramp up thermogenesis fast. That makes beige fat more like a reserve force than a fixed thermogenic depot.
Representative Peptide Pathways
Irisin is a myokine released from skeletal muscle during exercise. It acts on white adipocytes and induces UCP1 and other brown-fat genes, partly through PPARα activation and PGC-1α induction. In mouse studies, low-dose irisin promoted WAT browning and BAT activation, which reduced body weight by increasing heat production without changing food intake.
FGF21, produced mainly by the liver and thermogenic adipose depots, also supports this shift. It boosts UCP1 expression in WAT, activates PPARγ, and induces PGC-1α in adipose tissue and skeletal muscle. Put simply, both signals help recruit beige fat.
Target Tissues and Organ Axis
Browning happens mainly in subcutaneous WAT, including inguinal regions, where beige adipocytes appear inside white fat depots. Exercise-related signals and hepatic stress signals can both push WAT toward a beige phenotype.
Obesity-Treatment Relevance
This matters for obesity treatment because humans have limited BAT, but a lot of WAT. So instead of relying only on existing brown fat, one option is to convert part of white fat into thermogenic tissue. Preclinical data links this shift to better glucose tolerance and insulin sensitivity. That’s why browning is often viewed as a plausible add-on approach in obesity care.
The next mechanism shows how peptides coordinate this response across organs.
4. Endocrine Crosstalk
Unlike the first three mechanisms, endocrine crosstalk ties BAT to the liver, muscle, heart, and brain - and those organs send signals back to BAT too. That matters because BAT’s role in metabolism goes well beyond the adipocyte itself.
Key Signaling Loop
BAT also works as an endocrine organ. It releases BAT-derived signals, or batokines, such as FGF21, IL-6, and NRG4 to help coordinate thermogenesis and whole-body metabolism. The signal doesn’t move in just one direction, either. Other organs feed information back to BAT, creating a two-way loop.
In humans, 10 days of cold exposure increased FGF21 and BAT activity, with FGF21 strongly tracking peak BAT activity in adjusted analysis.
Representative Peptide Pathways
FGF21 sits close to the center of the liver–BAT axis and tracks with BAT activity in humans. Serum FGF21 was positively correlated with cold-induced BAT activity (r = 0.51, p = 0.01). Early clinical testing of the FGF21 analog LY2405319 has linked it to improved lipid profiles, lower fasting insulin, and reduced body weight.
GLP-1 receptor agonists may also increase sympathetic outflow to BAT and white fat. In plain English, they may add a thermogenic signal on top of their main appetite effect.
Target Tissues and Organ Axis
The main organ axes include:
- the liver–BAT axis (FGF21, NRG4, IL-6)
- the muscle–fat axis (irisin)
- the gut–brain–BAT axis (GLP-1)
BAT-derived NRG4 may reduce hepatic lipogenesis and steatosis.
Obesity-Treatment Relevance
For obesity care, this matters because BAT signaling can improve triglycerides, insulin resistance, and hepatic fat. That multi-organ effect helps explain why peptide therapeutics may matter even when BAT is not the main target.
The next section separates these peptide-linked signals from preclinical and human evidence.
How to Read the 4 Mechanisms in Clinical Practice
These mechanisms act at different points along the same pathway. That simple framework makes the peptide examples in the next section much easier to read.
How UCP1 Differs From the Other Mechanisms
UCP1 is the direct thermogenic switch. It’s the final heat-producing step, so changes here are the clearest sign that thermogenesis has turned on.
When a peptide shifts UCP1 expression or activity, you’d expect the most immediate effect on resting energy expenditure. That said, direct UCP1 activity still depends on mitochondrial capacity to keep heat output going.
How Mitochondrial Remodeling Supports Heat Output
Mitochondrial remodeling supports that switch. Put plainly, it sets the thermogenic ceiling. If mitochondrial function is weak, UCP1 has less capacity to sustain heat output.
The main issue here is thermogenic capacity. Interventions that improve mitochondrial biogenesis or oxidative capacity can increase energy expenditure and nutrient disposal. Over time, that may help fasting glucose and triglycerides. But these shifts usually show up gradually, so they point more to capacity than to immediate activation.
How Browning Expands Thermogenic Capacity
Browning is a capacity-building mechanism, not an acute activator. It expands the pool of heat-producing cells, but those cells still need UCP1 and mitochondrial readiness to do the job.
So if a peptide increases browning capacity, expect delayed body-composition changes instead of near-term shifts in REE. Obesity can blunt this conversion and reduce thermogenic reserve.
How Endocrine Crosstalk Coordinates Multi-Organ Effects
At the systems level, endocrine crosstalk links BAT to whole-body metabolism. This layer helps explain why metabolic gains can be bigger than what BAT scans or direct BAT measures seem to show.
When a peptide works through this pathway, don’t look at BAT alone. Use a full metabolic panel. Changes in insulin sensitivity, triglycerides, and hepatic fat may appear even when direct BAT activity changes are modest.
Clinical Relevance for Obesity Care
In practice, these mechanisms point to different response patterns. Proper patient selection criteria are essential to ensure these metabolic shifts align with clinical goals. Across all four, the obesity-related endpoints overlap:
- Resting energy expenditure
- Body fat
- Glycemia
- Triglycerides
- Waist circumference
A peptide that mainly activates UCP1 may have the clearest effect on REE and near-term weight loss. One that mainly drives browning or mitochondrial remodeling may show slower shifts in body composition and metabolic markers over weeks to months.
Endocrine modulators can produce multi-organ metabolic effects, sometimes out of proportion to measurable BAT activity. That’s why they should be judged with a full metabolic panel, not REE alone. The next section maps these layers to GLP-1, FGF21, and irisin-related pathways.
Peptide Examples and Translational Notes
GLP-1RAs have the strongest clinical footing. FGF21 and irisin are still more translational than established.
The clearest clinical example is GLP-1, since it already shows up in approved obesity treatment.
GLP-1 Pathways and Brown Fat Signaling
Through endocrine crosstalk, GLP-1RAs have shown clear obesity benefit. Their BAT signal is still being worked out. In a 12-week exenatide study, researchers saw a 28% increase in metabolic BAT volume and an 11% rise in SUVmean on FDG-PET/CT. That said, the main upside of these drugs is still appetite suppression and cardiometabolic improvement. BAT activation is an exploratory effect, not the clinical target.
FGF21 is the clearest case of a pathway that links endocrine crosstalk to browning and mitochondrial support.
FGF21-Related Signaling
FGF21 sits at the overlap of endocrine crosstalk, browning, and mitochondrial mechanisms. In humans, serum FGF21 correlates with cold-induced BAT activity and acts as a strong determinant of maximal BAT activation under cold stimulation. FGF21 analogs are in early clinical development for metabolic disease. Right now, their positioning is focused on glycemic control and cardiometabolic risk.
Irisin is the most direct browning example, but the human data still shifts around more than you'd want.
Irisin-Associated Browning Biology
Irisin is tied directly to adipocyte browning. In human white adipocytes, irisin treatment increased the share of UCP1-positive cells from 12% in controls to 57%, along with 1–3-fold increases in UCP1 protein. Even so, the human evidence remains inconsistent. Assay variability and reproducibility problems still limit its standing as an established clinical target.
Preclinical vs. Human Evidence
The table below separates approved signals from early-development and uncertain ones. That split matters. A molecule can change BAT-related pathways in the lab and still fall short where it counts: weight, glycemic, or metabolic benefit in actual patients. In practice, clinical use should still track weight, A1C, triglycerides, and hepatic fat.
| Pathway | Preclinical Evidence | Human Translational Evidence | Clinical Status |
|---|---|---|---|
| GLP-1RAs | BAT activation, WAT browning in rodents | +28% BAT metabolic volume on PET/CT (exenatide, 12 weeks) | Approved for obesity/T2D; BAT effect exploratory |
| FGF21 | BAT activation, UCP1-dependent browning | Correlates with cold-induced BAT activity | Analogs in early development |
| Irisin | Strong WAT browning, UCP1 induction | Inconsistent; assay variability | Not an established clinical target |
A Resource Note for U.S. Prescribers
These mechanisms are still making their way into day-to-day care. So for prescribers, it helps to have a practical reference close at hand.
For licensed U.S. prescribers, PeptidePrescriber offers reference materials that help bridge peptide biology and clinic-ready decision-making. The platform includes monographs, dosing protocols, calculators, injection guides, and regulatory references in a pharmacy-agnostic format. Clinicians can use it to check dosing, review injection technique, and look at regulatory points before prescribing.
If you're new to peptide therapy, the Starter Pack includes consent templates, an implementation checklist, and a regulatory quick reference. In plain terms, that makes it most useful as a clinical reference tool, not as a mechanism claim.
Comparison Table: 4 Mechanisms at a Glance
4 Brown Fat Activation Mechanisms: Peptide Pathways Compared
These four mechanisms don’t all work in the same place, and they don’t act on the body in the same way either. Some target brown fat directly, some push cells to burn more fuel, and some work through signals passed between organs. The table below lines them up by tissue target, signal type, strength of evidence, and why they matter for obesity treatment.
| Mechanism | Thermogenic Pathway | Primary Tissues | Peptide/Signal Examples | Evidence Level | Obesity-Treatment Relevance |
|---|---|---|---|---|---|
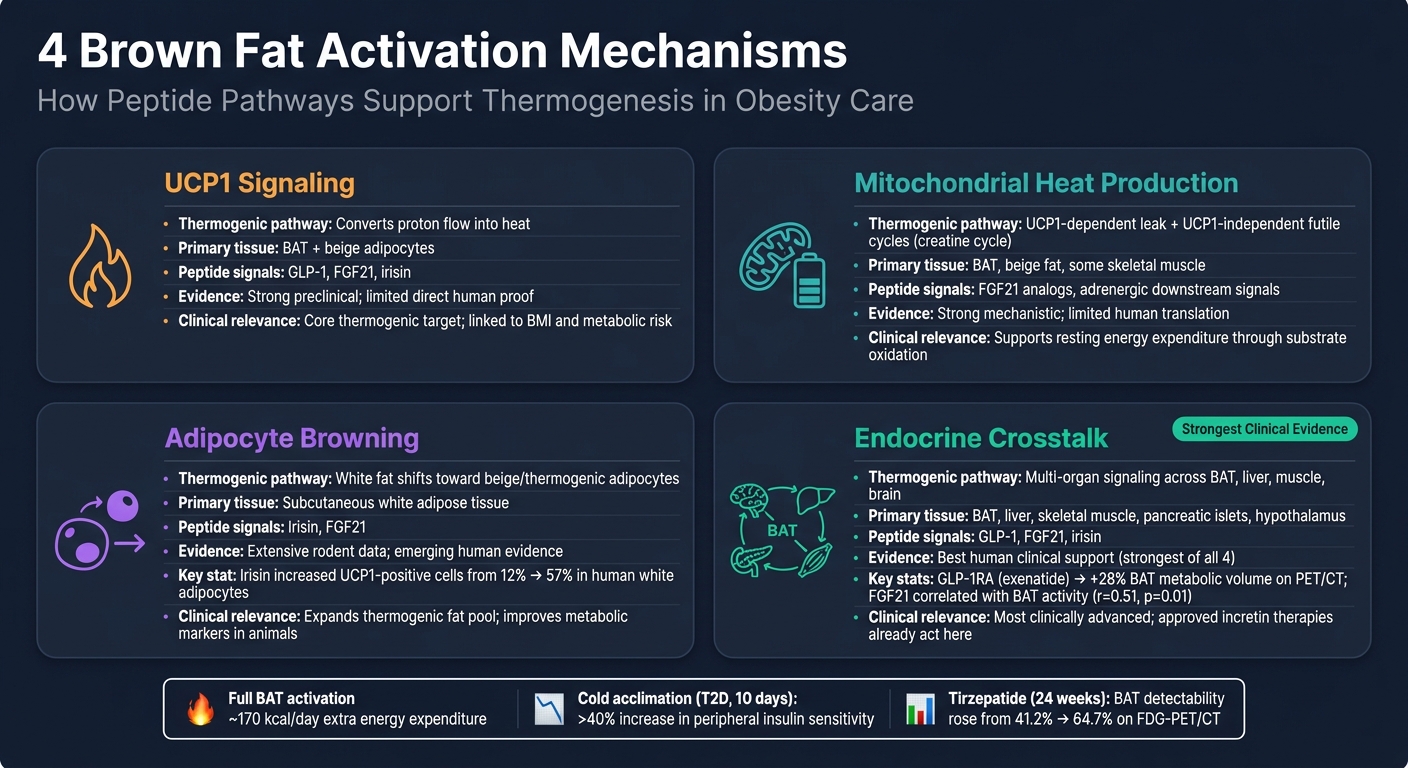
| UCP1 Signaling | UCP1 converts proton flow into heat | BAT, beige adipocytes | GLP-1, FGF21, irisin | Strong preclinical data; human correlation studies. | Core thermogenic target linked to BMI and metabolic risk. |
| Mitochondrial Heat Production | UCP1-dependent leak and UCP1-independent futile cycles | BAT and beige fat, with some skeletal muscle involvement | FGF21 analogs; adrenergic downstream signals | Strong mechanistic data; limited human translation. | Supports energy expenditure through substrate oxidation. |
| Adipocyte Browning | White fat shifts toward beige, thermogenic adipocytes | Subcutaneous white adipose tissue depots | Irisin, FGF21 | Extensive rodent data; emerging human evidence. | Expands thermogenic fat and improves metabolic markers in animals. |
| Endocrine Crosstalk | Multi-organ signaling across BAT, liver, muscle, and brain | Brown and beige fat, liver, skeletal muscle, pancreatic islets, hypothalamus | GLP-1, FGF21, irisin | Best human clinical support; BAT-specific effects remain indirect. | Most clinically advanced because approved incretin therapies already act here. |
Endocrine crosstalk has the strongest clinical footing right now. The other three are still driven more by mechanistic and preclinical work, even though they point to clear paths for obesity therapy.
Conclusion
Peptide-driven brown fat activation works through four connected pathways: UCP1 signaling, mitochondrial heat production, adipocyte browning, and endocrine crosstalk. What matters in the clinic is simple: how much extra thermogenic capacity these pathways add.
Taken together, these mechanisms may help with obesity care by increasing energy expenditure, improving insulin sensitivity, and supporting glucose and lipid metabolism. Brown fat activation and browning are not the same thing, but they can work side by side. Still, even with full activation, the gain in human energy expenditure looks modest. So it makes more sense to treat these pathways as supportive add-ons, not stand-alone treatments. The evidence base is also uneven, and much of the direct peptide research aimed at brown fat is still mechanistic or preclinical. That’s why the quality of the evidence matters so much in day-to-day care.
For U.S. prescribers, these pathways can serve as a practical framework for judging evidence quality, patient fit, and regulatory status before any discussion of investigational peptide use. In practice, the aim is realistic use, not hype.
These four mechanisms give clinicians a clear way to assess new data and set grounded expectations for peptide therapies.
FAQs
Can brown fat activation meaningfully help with weight loss?
Brown fat activation may help with weight loss because it increases thermogenesis and overall energy use. Put simply, brown adipose tissue burns stored fat to make heat, and that can support weight management.
That said, its strongest role seems to be as part of a multi-modal approach. Right now, support mostly comes from preclinical findings and mechanistic evidence, not strong human outcome data alone.
What is the difference between brown fat and beige fat?
Both brown fat and beige fat make heat through mitochondrial thermogenesis, but they don't come from the same place or follow the same rules.
Brown fat is built into the body as part of normal development and shows up in specific locations. Beige fat, by contrast, is inducible. It forms inside white fat through a process called browning, often in response to outside conditions or peptide-based signals.
Which peptides have the best human evidence for brown fat effects?
Currently, no peptide has strong, clear human clinical evidence proving that it directly activates brown adipose tissue.
That said, some agents that target GLP-1, GIP, or glucagon receptors may influence energy expenditure and lipolysis through other mechanisms. In plain English: they may still affect how the body uses and burns energy, just not in a way that's been clearly shown to directly switch on brown fat in humans.
There are also investigational compounds like 5-Amino-1MQ. Early preclinical results look promising, but there's a catch: human clinical trial data isn't there yet.