
There is no standard oxytocin dose for social impairments. Across studies, I see intranasal dosing from 8 IU to 80 IU, with 24 IU used most often, but results stay mixed.
If I had to boil the article down fast, it comes to this:
- 24 IU is the main reference dose in research
- 48 IU/day has the clearest pooled signal in ASD trials
- 8 IU to 80 IU/day has been tested overall
- Single-dose studies and multi-week studies should not be read the same way
- A large 24-week pediatric trial found no clear difference from placebo
- Safety follow-up should include baseline CMP and serum sodium, then repeat sodium at 2 to 4 weeks
In other words: if you’re reviewing oxytocin use for social impairment, I would not ask only, “What dose was used?” I would also check who got it, how often, for how long, and what outcome was measured.
Oxytocin Administration, Neural Sensitivity, and Autism
sbb-itb-7164bd9
Quick comparison
| Framework | Common dose pattern | Usual goal | What I’d keep in mind |
|---|---|---|---|
| Acute single dose | Often 24 IU once | Short-term social-cognitive effects | Not built for long-term symptom change |
| Repeated daily dosing | 16 IU to 48 IU/day in many ASD trials | Day-to-day social behavior | Mixed results across studies |
| Step-up dosing | 8 IU to 80 IU/day | Tolerability and dose build-up, often in youth | Separate starting, target, and delivered dose |
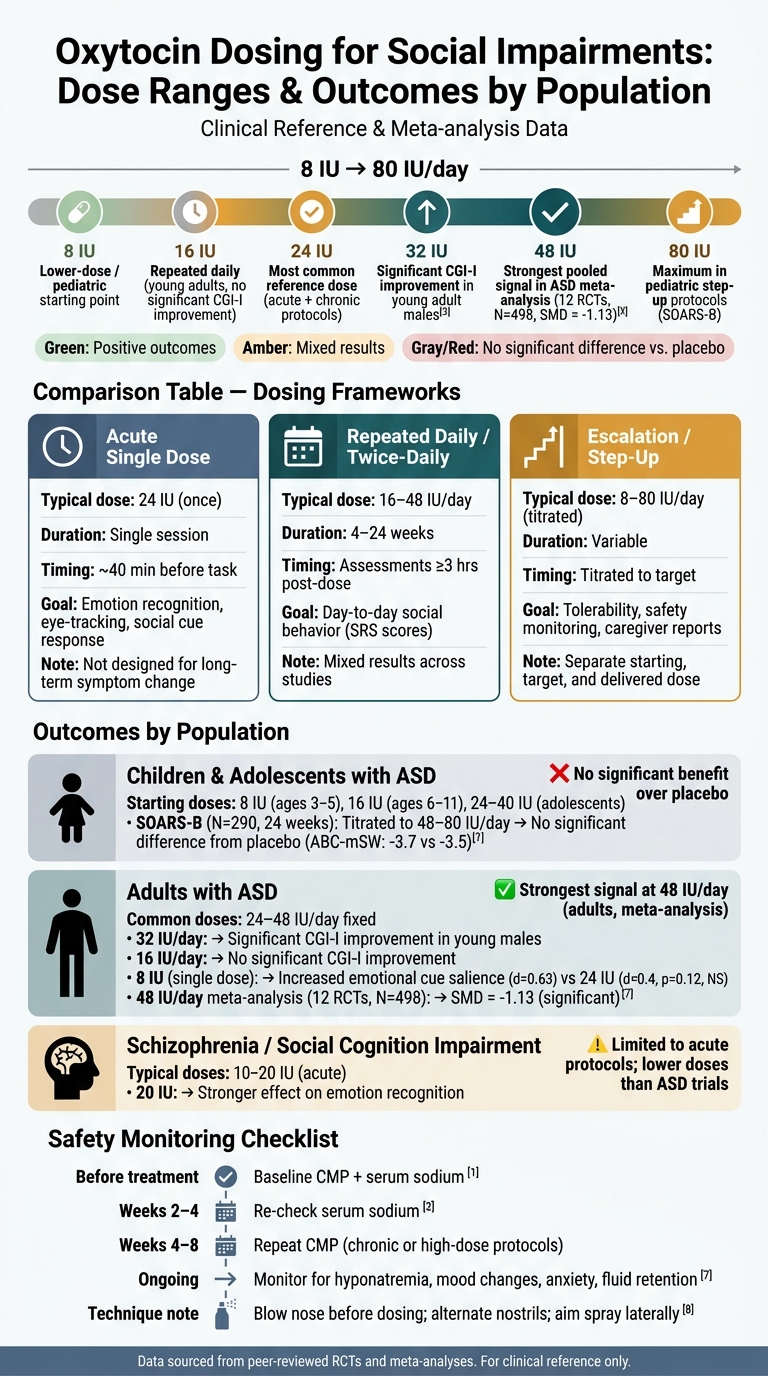
A few points stand out from the data. In one adult ASD crossover trial, 8 IU beat 24 IU on emotional-cue salience. In young adults with ASD, 32 IU/day showed better CGI-I results than 16 IU/day. But in children and teens, even titration up to 48 to 80 IU/day did not beat placebo over 24 weeks in SOARS-B.
So my read is simple: oxytocin dosing has to be matched to the study design and patient group, not copied from one paper to another. The article supports use as a carefully tracked adjunct, with close attention to nasal technique, timing, sodium checks, and behavior changes.
Step 1: Identify the dosing framework used in the literature
Before you apply oxytocin trial data to a patient, sort each study into one of three buckets: acute, repeated, or step-up. That comes first.
Why? Because an acute challenge study and a repeated treatment protocol are trying to answer different things. If you treat them like they mean the same thing, your read on dose, timing, and likely results can get off track fast.
"Discrepancies between reports of single-dose and continuous treatment with different doses and frequencies were observed in previous studies; these factors can directly influence detecting the effects of OXT treatment." - Yingying Zhang, Ulm University
Acute single-dose protocols
Acute protocols are short-term experimental setups. They use one intranasal dose to measure near-term changes, such as emotion recognition, eye gaze, or responses to social cues.
That matters because these studies are not built to test long-term symptom change. So if you pull dose data from an acute study and use it to guide a long-course treatment plan, you end up with a design mismatch. And that can skew both expectations and follow-up decisions.
Repeated daily and twice-daily protocols
Repeated-course protocols usually run for 4 to 24 weeks. They use once-daily or twice-daily dosing to track cumulative change in day-to-day social behavior.
These studies often rely on caregiver-rated tools like the Social Responsiveness Scale (SRS), with assessments done at least 3 hours after the last dose. Adherence also becomes a bigger issue here than in single-dose studies. Some trials check actual use by weighing bottles before and after dosing, which is worth paying attention to when you judge how solid the dosing data is.
Escalation and step-up dosing methods
Some pediatric studies use gradual titration. They start low, then move up over time until they reach a target dose.
This approach is especially relevant in children and adolescents, where tolerability and safety checks come first, often requiring practical guides for proper administration. One large 24-week trial used an age-adjusted flexible schedule ranging from 8 IU to 80 IU daily. In these studies, don't lump all dosing into one number. Separate the starting dose, target dose, and average delivered dose.
| Framework | Typical Duration | Dose Timing | Primary Outcome Focus |
|---|---|---|---|
| Acute challenge | Single session | ~40 min pre-task | Emotion recognition, eye-tracking, response to social cues |
| Repeated daily/twice-daily | 4–24 weeks | ≥3 hrs post-dose for assessments | SRS scores, repetitive behavior scales |
| Escalation/step-up | Variable | Titrated to target | Safety monitoring, tolerability, caregiver reports |
For more clinical insights on emerging research, With the framework clear, the next move is to compare dose ranges and outcomes in Step 2.
Step 2: Review the Studied Dose Ranges and Outcomes
Oxytocin Dosing for Social Impairments: Dose Ranges, Populations & Outcomes
Tested doses run from 8 IU to 80 IU/day, and the results don't move in a neat straight line from low dose to high dose. So it makes sense to start at the low end, then look at how those findings stack up against the 24 IU benchmark and the higher-dose plans.
Lower-dose protocols: 8 IU and 24 IU comparison
One of the most useful lower-dose findings comes from a crossover trial in adults with ASD. In that study, a single 8 IU dose significantly increased the salience of emotional cues (d = 0.63), while a 24 IU dose in the same trial did not reach statistical significance (d = 0.4, p = 0.12).
That result is a good reminder that dose isn't the whole story. The study used an optimized nasal delivery device, which may have improved deposition and helped the 8 IU dose work better. Put simply, you can't look at dose in isolation. Route and regimen matter too. Clinicians can access prescribing guidance to better understand these delivery nuances.
The most commonly studied protocol: 24 IU
24 IU is often the main reference point for comparing lower and higher-dose plans. It's usually given as 6 sprays at 4 IU each. Even so, the results at 24 IU are mixed and shift based on diagnosis, age, and the outcome being measured.
In young adults with ASD, doses above 21 IU/day were more effective than lower doses for improving Clinical Global Impression-Improvement (CGI-I) scores. That's a useful threshold to keep in mind when 24 IU is used as a starting point in adult protocols.
Higher-dose protocols: 48 IU per day and flexible regimens
At the higher end, 48 IU/day - usually 24 IU twice daily - showed benefit in meta-analysis. A 2025 meta-analysis of 12 RCTs involving 498 patients found a significant improvement in social impairments with 48 IU/day (SMD = -1.13).
But the picture gets murkier in large pediatric trials. The SOARS-B trial, published in the New England Journal of Medicine, used a flexible titration schedule that started at 8 IU and aimed for 48 IU daily, with some participants going up to 80 IU/day (mean maximal dose, approximately 67.6 IU). Over 24 weeks in 290 children and adolescents, the mean change in social withdrawal scores was almost the same in the oxytocin and placebo groups (-3.7 vs. -3.5), with no significant difference on the ABC-mSW scale.
| Dose (Daily) | Frequency | Population | Duration | Observed Social Outcomes |
|---|---|---|---|---|
| 8 IU | Single dose | Adults with ASD | Acute | Increased salience of emotional cues; reduced amygdala activation |
| 16 IU | Once daily | Young adults with ASD | 12 weeks | No significant improvement in CGI-I scores vs. placebo |
| 24 IU | Once or twice daily | Adults with ASD | Varied | Most common reference regimen; mixed results |
| 32 IU | Once daily | Young adults with ASD | 12 weeks | Significant improvement in CGI-I scores in male participants |
| 48 IU | 24 IU twice daily | Mixed ASD cohorts | Various | Significant improvement in social impairments in meta-analysis |
| 48–80 IU | Titrated daily | Children and adolescents with ASD | 24 weeks | No significant difference from placebo on the ABC-mSW scale |
These dose-response patterns change by age and diagnosis. That's why Step 3 looks at pediatric ASD, adult ASD, and schizophrenia cohorts separately.
Step 3: Match the Protocol to the Patient Population
Use what you mapped in Steps 1 and 2 to fit the dose to the patient’s age, diagnosis, and treatment length. The dose-response patterns from Step 2 don’t play out the same way in every group. Age, diagnosis, and sex can all change how someone responds to the exact same dose.
Children and Adolescents with Autism Spectrum Disorder
For children and adolescents with ASD, age-adjusted stepwise escalation is used more often than a single fixed dose. Starting points are 8 IU for ages 3–5, 16 IU for ages 6–11, and 24–40 IU for adolescents. Younger children may respond more strongly to lower doses, and some studies use a placebo lead-in phase to account for expectancy effects.
The SOARS-B trial followed this escalation approach. It aimed for 48 IU daily, with a ceiling of 80 IU, and found no significant difference from placebo over 24 weeks.
As patients get older, protocols tend to move away from flexible escalation and toward fixed daily dosing.
Adults with Autism Spectrum Disorder
In adults with ASD, fixed daily regimens of 24 to 48 IU are more common than escalation protocols. Among young men, 32 IU/day has the clearest signal. It showed significant CGI-I improvement over placebo, while 16 IU/day did not reach significance.
OXTR genotype may also shape response, especially at doses of 21 IU/day or less.
Evidence in schizophrenia-spectrum groups looks different. It is usually more acute and uses lower doses than ASD trials.
Schizophrenia and Other Social Cognition Impairment Cohorts
Schizophrenia-spectrum studies usually rely on acute dosing in the 10- to 20-IU range, with 20 IU showing the stronger effect on emotion recognition. After choosing the right population, the next step is safety monitoring and documentation.
Safety, monitoring, and key takeaways
Once the dose matches the patient group, the next step is safety, monitoring, and clean documentation.
Monitoring points during oxytocin treatment
In most trials, adverse event rates look similar to placebo. In the 24-week SOARS-B trial ((N=290)), there were no significant differences in serious adverse events. That said, sodium needs close follow-up. Oxytocin can cause hyponatremia, and in rare cases that can progress to seizures or coma.
A simple lab plan helps:
- Get a baseline Comprehensive Metabolic Panel (CMP) and serum sodium before treatment starts
- Re-check serum sodium at 2–4 weeks
- Repeat the CMP at 4–8 weeks in chronic or high-dose protocols
Use sodium trends, tolerability, and clinical response to decide whether to escalate, maintain, or stop treatment. Labs matter, but behavior matters just as much.
About 75% of patients with ASD have psychiatric comorbidities such as anxiety or ADHD, which can blur the line between treatment effects and baseline symptoms. Regular patient or caregiver diaries can help track mood, irritability, sleep, and arousal. Watch for paradoxical increases in anxiety or social vigilance, especially in ambiguous or threatening settings. If the patient develops severe headache, nausea, mood swings, or fluid retention, adjust the plan or stop treatment.
Intranasal delivery also depends heavily on technique. Bioavailability is low, so small mistakes can change the response. Patients should blow the nose before dosing, alternate nostrils, and aim the spray laterally along the nasal wall.
How to document protocol choice and follow-up
Clinical notes should spell out the intranasal route, dose in IU, frequency, and the behavioral context around dosing. If you're measuring acute social effects, time doses 30–45 minutes before assessments or therapy. That timing should be documented clearly, because it can shape the response you see.
Target outcomes should be tied to validated tools. The Social Responsiveness Scale (SRS-2) is the main measure for social impairment severity, while the Repetitive Behavior Scale-Revised (RBS-R) tracks restricted interests. Reassess after 4 weeks, then again 4 weeks after cessation to see whether any gains last. When the plan changes, document why. The note should include the rationale for escalation, continuation, or discontinuation based on response and tolerability, not just the new dose.
Key takeaways for clinicians
| Takeaway | Detail |
|---|---|
| Intranasal route remains the standard study route | All major social impairment trials use intranasal delivery |
| 24 IU remains the reference dose for comparison and documentation | Used across acute and chronic protocols in ASD and schizophrenia research |
| Lower doses have been studied in young children | 8 IU per dose has been studied in children ages 3–5 |
| 48 IU/day has the strongest pooled signal in ASD trials | A meta-analysis of 12 RCTs found a beneficial effect at 48 IU per day in ASD |
| No single dose or schedule is established | Dose, schedule, and population must be matched together |
Trial results are still mixed, so oxytocin fits best as a matched adjunct rather than a universal treatment.
FAQs
How do I choose between acute, daily, and step-up dosing?
The right approach depends on the clinical goal.
Acute dosing is usually given 30 to 45 minutes before a specific social task or therapy session. Daily dosing is used in 4- to 12-week protocols for ongoing social impairments. In some cases, clinicians use cycles as a precaution.
Step-up dosing is not a standard oxytocin protocol. Response can vary from person to person, and higher doses don't always work better. Because of that, clinicians often begin with a standard 24 IU intranasal dose and watch outcomes before making any changes.
Why might 48 IU/day help in some ASD studies but not in children?
Results are mixed because ASD is highly heterogeneous. In plain English, people with ASD can differ a lot from one another, so the same treatment may help one group and do little for another.
Meta-analyses suggest that 48 IU/day may help with social impairments in adults. In children, though, the findings are still equivocal.
There are a few likely reasons for that:
- Small study size
- Differences in treatment duration
- Differences in outcome measures
- Biological factors such as baseline oxytocin levels, receptor genotype, and age-related responses
That mix can make results hard to compare across studies, and it may help explain why the picture still looks uneven.
What monitoring is most important during oxytocin treatment?
Monitoring should center on safety and possible physiologic effects.
The big one is electrolytes - especially sodium. Oxytocin has antidiuretic properties, so it can increase the risk of hyponatremia.
Baseline labs should also cover kidney and liver function. From there, periodic hormone panels can help track how things are shifting over time, including:
- Estradiol
- Progesterone
- Testosterone
Clinicians should also watch for possible receptor desensitization with chronic use.