
Recovering from surgery faster is possible with the right peptide therapy. BPC-157 and TB-500, two widely studied peptides, are used to support healing by enhancing blood flow, cell migration, and tissue repair. These peptides, often combined as the "Wolverine Stack", have reportedly reduced recovery times by up to 50% when used alongside physical therapy and proper post-operative care.
Key points to know:
- BPC-157 promotes blood vessel formation and collagen repair.
- TB-500 aids systemic cell migration and reduces scar tissue formation.
- Therapy must be supervised by a licensed professional and follow strict dosing timelines.
- Contraindications include active cancer, pregnancy, and certain medications.
- Proper sourcing, informed consent, and monitoring are critical for safety.
This guide outlines how to time and dose these peptides effectively, ensuring they complement your body’s natural healing process without replacing essential rehabilitation efforts.
What Is the Wolverine Stack? BPC-157, TB-500 and the Evidence
Before You Start: Prerequisites for Peptide Therapy
Before diving into the dosing protocols, it's crucial to ensure that all conditions for starting peptide therapy are met. This means conducting a thorough screening process, confirming patient eligibility, securing proper regulatory documentation, and completing a detailed baseline assessment. These steps are non-negotiable for safe and effective use of peptides like BPC-157 and TB-500.
Patient Eligibility and Contraindications
Peptide therapy is best suited for adults (18 and older) recovering from musculoskeletal or reconstructive surgeries. This includes procedures like ACL reconstructions, joint replacements, or even cosmetic surgeries such as abdominoplasty. However, therapy must be overseen by a licensed MD or APRN with expertise in regenerative medicine.
There are certain conditions where peptide therapy is strictly off the table. For instance, patients with active malignancies or those who have recently undergone cancer surgery should avoid these peptides. Both BPC-157 and TB-500 encourage angiogenesis, which could potentially aid tumor growth. Other contraindications include pregnancy, breastfeeding, active surgical site infections, and allergies to peptides or bacteriostatic water.
Medication reviews are another essential step. Drugs like anticoagulants, immunosuppressants, and diabetes medications need careful evaluation since they can affect blood flow and glucose regulation. Additionally, competitive athletes require extra caution. TB-500 is on the WADA prohibited list, and BPC-157 is also banned for clinical use in sports. These factors must be addressed before moving forward.
Regulatory Compliance and Informed Consent
Patients need to be fully informed - and sign documentation acknowledging - that BPC-157 and TB-500 are not FDA-approved as finished drug products and are being used off-label. This step isn’t just about covering legal bases; it helps manage expectations and protects both the patient and the prescriber.
Equally important is sourcing. Always obtain peptides from licensed 503A compounding pharmacies. These facilities ensure sterility, perform identity testing, and provide lot-specific certificates of analysis.
"Post-surgical patients have lower margin for vial contamination than recreational users. Source through a 503A compounding pharmacy under prescription wherever possible." - Chris Hallewell, Founder, Underground Biohacking
The informed consent process should also make it clear that no specific outcomes are guaranteed, ensuring transparency from the outset.
Baseline Assessment and Preparation
Before the first injection, it’s essential to document the patient’s condition. Record pre-surgical pain levels, the status of wounds or incisions, and baseline range of motion. Preoperative imaging, such as MRIs or ultrasounds of the surgical site, should be on hand. Additionally, order a full metabolic panel, Vitamin D levels (aiming for 50–70 ng/mL), iron studies, and immune markers like IL-6 and TNF-alpha. If growth hormone secretagogues such as Ipamorelin are part of the plan, measure baseline levels of IGF-1, fasting glucose, and fasting insulin.
Clearance from the surgical team is mandatory before starting therapy. Administering peptides too soon - within 24 hours post-surgery - can disrupt normal clot formation, especially with TB-500. For more complex procedures, it may be best to wait one to two weeks until the acute inflammatory phase has passed.
Finally, ensure staff are trained in aseptic techniques for reconstituting and administering subcutaneous injections. Proper site rotation is another key detail to cover. These steps lay the groundwork for safe and effective peptide therapy and set the stage for the dosing protocols that follow.
BPC-157 Dosing Checklist for Post-Surgical Healing
Indications and Dosing Guidelines
This protocol outlines the use of BPC-157 for soft-tissue repair, focusing on tendons, ligaments, and muscles - common areas affected by surgeries like ACL reconstructions, rotator cuff repairs, or Achilles tendon procedures. BPC-157 is known to promote angiogenesis and enhance collagen deposition at the repair site.
The dosing strategy is phased, with simpler repairs requiring 4–6 weeks and more complex reconstructions extending to 8–12 weeks, depending on recovery progress:
| Phase | Duration | Dose | Frequency | Primary Goal |
|---|---|---|---|---|
| Acute/Loading | Weeks 1–2 | 500 mcg | Twice daily | Vascular repair & inflammation control |
| Maintenance | Weeks 3–8 | 250 mcg | Once daily | Collagen deposition & tissue building |
| Remodeling | Weeks 9–12+ | 250 mcg | Once daily | Fiber alignment & functional strength |
For patients over 40, combining BPC-157 with a growth hormone secretagogue like Ipamorelin may further enhance collagen synthesis, particularly in cases of declining growth hormone levels.
Administration and Timing
The standard delivery method for BPC-157 is subcutaneous injection. For surgeries involving superficial structures, such as the Achilles or patellar tendons, injecting near the surgical site increases local tissue concentrations. For deeper structures, like the rotator cuff, systemic injections (e.g., in the abdomen) are a practical alternative.
Important Note: Never inject directly into a tendon or open wound. Always inject near the site to avoid disrupting the structural integrity or increasing the risk of infection.
Timing is another critical factor. BPC-157 should be initiated 24–72 hours after surgery, once primary hemostasis is confirmed. Starting earlier could interfere with the formation of the initial clot. For gastrointestinal surgeries, many clinicians recommend waiting 48 hours post-op to ensure the surgical seal is secure.
Nutritional support is also key during this period. Aim for 1.6–2.0 g of protein per kilogram of body weight and 2,000 mg of Vitamin C daily to aid collagen cross-linking. Additionally, avoid NSAIDs, as they can disrupt the early inflammatory response that BPC-157 supports.
Consistent monitoring ensures the protocol is followed correctly, and doses are adjusted as needed.
Monitoring and Dose Adjustments
Weekly check-ins are essential to assess pain levels, range of motion, swelling, and the incision's appearance. Formal evaluations should occur at weeks 2, 4, 8, and 12, with imaging (ultrasound or MRI) at weeks 8–12 to confirm structural integrity before resuming full activity.
Chris Hallewell highlights an important point:
"BPC-157 reduces pain ahead of structural readiness. That gap is where re-injury lives."
This underscores the importance of continuing physical therapy and progressing cautiously, even if pain subsides, as structural healing takes time.
Red flags that require immediate attention or dose adjustments include persistent redness or heat at the incision site beyond Day 7, foul-smelling discharge, a sudden plateau in range of motion, or systemic symptoms like dizziness or lethargy. If infection is suspected, stop using BPC-157 and consult the surgical team, as the peptide does not address bacterial infections.
TB-500 Dosing Checklist and Stacking with BPC-157
Indications and Role of TB-500
TB-500 is a synthetic fragment derived from Thymosin Beta-4, which is the most abundant intracellular peptide found in the human body. Unlike BPC-157, which focuses on localized angiogenesis and wound healing, TB-500 works on a systemic level. It mobilizes repair cells to injury sites through pathways involving actin remodeling. This makes it especially useful for complex orthopedic recoveries, such as ACL reconstructions, rotator cuff repairs, or other major soft-tissue surgeries, where healing needs extend beyond the immediate surgical site. However, TB-500 is not recommended for individuals with active malignancies.
Dosing and Administration
TB-500 dosing follows a two-phase approach: a loading phase and a maintenance phase.
- Loading Phase (Weeks 1–4): Administer 2.5–5 mg twice weekly (e.g., Monday and Thursday).
- Maintenance Phase (Weeks 5–8): Reduce the dose to 2–2.5 mg once weekly. Some clinicians may stop after the loading phase if recovery is progressing well.
| Phase | Duration | Dosage | Frequency |
|---|---|---|---|
| Loading | Weeks 1–4 | 2.5–5 mg | Twice weekly |
| Maintenance | Weeks 5–8 | 2–2.5 mg | Once weekly |
TB-500 is injected subcutaneously into abdominal fat. To prepare, reconstitute the peptide using bacteriostatic water (5 mg/mL concentration). Direct the water gently onto the vial wall and swirl it to mix - avoid shaking. Once reconstituted, store the vial in the refrigerator at 35–46°F. The solution remains stable for about 1–2 weeks.
With these dosing guidelines in place, combining TB-500 with BPC-157 can create a powerful recovery stack.
Stacking Protocols and Monitoring
The combination of BPC-157 and TB-500, often referred to as the "Wolverine Stack", is designed to optimize healing. While BPC-157 focuses on local vascular repair, TB-500 complements it by promoting systemic cell migration. A common stacking protocol involves BPC-157 at 250–500 mcg daily alongside TB-500 at 2.5–5 mg twice weekly during the loading phase.
"BPC-157 builds new vessels while TB-500 mobilizes repair cells - together, they act synergistically." - Dr. Agullo, Double Board-Certified Plastic Surgeon
When using this stack, always draw the peptides into a single syringe only at the time of injection. Store each peptide in its original vial, as their stability timelines differ. It's worth noting that, as of 2025, there are no published clinical trials for this specific combination - current evidence comes from preclinical studies. Despite this, some surgeons report that patients using this stack recover in about half the expected time.
Patients should carefully monitor injection sites for signs of infection, such as heat, redness, or discharge. Additionally, tracking pain levels, range of motion, and swelling during the loading phase can help determine when to transition into the maintenance phase. Dr. Julian Douwes, M.D., emphasizes the importance of rehabilitation alongside peptide therapy:
"A patient who receives BPC-157 and TB-500 but does not do their physical therapy will not recover as well as a patient who does their physical therapy without peptides. The rehabilitation is the foundation. The peptides are the adjunct."
While the stack may quickly reduce pain, it’s crucial not to skip physical therapy or exceed the surgeon’s prescribed guidelines for recovery.
sbb-itb-7164bd9
Post-Surgery Peptide Protocol Checklist by Procedure Type
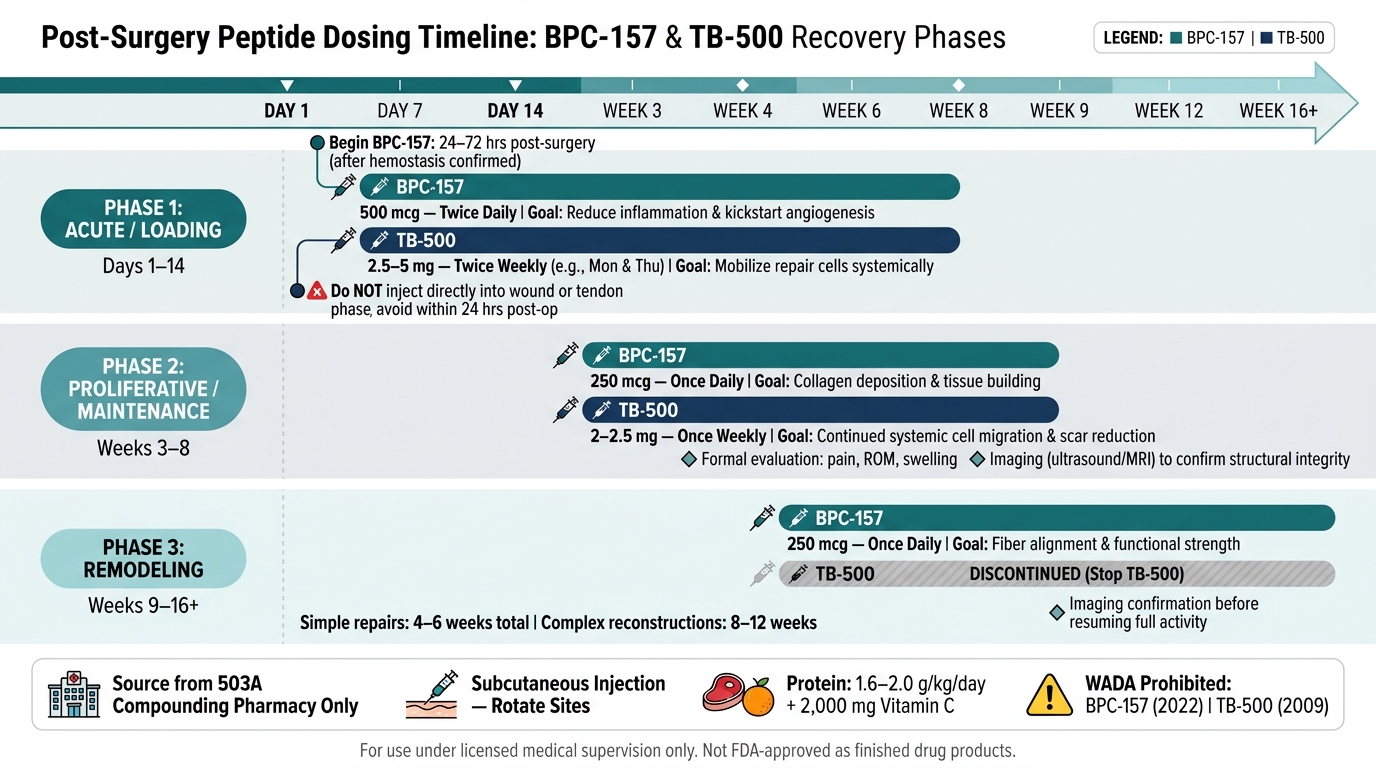
Post-Surgery Peptide Dosing Timeline: BPC-157 & TB-500 Recovery Phases
When it comes to post-surgery recovery, tailoring peptide protocols to the specific type of procedure can make a big difference. For example, the needs of someone recovering from ACL reconstruction are quite different from those of a patient undergoing body contouring. The key to improving recovery lies in matching the right peptides to the right procedure at the right time.
Procedure-Specific Protocols
Here’s a breakdown of peptide protocols for various surgical procedures:
| Procedure Type | Primary Peptides | Typical Dosing | Duration |
|---|---|---|---|
| Orthopedic (Joint/Ligament) | BPC-157 + TB-500 | BPC-157: 250–500 mcg twice daily; TB-500: 2.5–5 mg twice weekly | 6–12 weeks |
| Spinal Surgery | BPC-157 + TB-500 | BPC-157: 500 mcg twice daily; TB-500: 2.5 mg twice weekly | 8–12 weeks |
| Body Contouring (Tummy Tuck, Liposuction) | BPC-157 + TB-500 + GHK-Cu (collagen stimulation) + KPV (anti-inflammatory) | Daily compounded blend injection | 4–6 weeks |
| Facial Plastic Surgery | BPC-157 + TB-500 + GHK-Cu (collagen stimulation and skin repair) | Daily compounded blend injection | 3–4 weeks |
| Abdominal/GI Surgery | BPC-157 (primary) | 250–500 mcg twice daily | 4–8 weeks |
For orthopedic and spinal surgeries, the focus is on supporting tendon and bone healing while minimizing inflammation. In these cases, BPC-157 is injected subcutaneously near the surgical site (but not directly into the incision), while TB-500 is administered systemically, usually in the abdominal area.
Body contouring procedures often trigger a broader inflammatory response. To address this, KPV (Lysine-Proline-Valine) is added to the peptide mix, alongside BPC-157, TB-500, and GHK-Cu. For abdominal or gastrointestinal surgeries, BPC-157 is prioritized for its protective effects on the digestive system. It’s typically introduced 48 hours post-surgery to give the surgical site time to seal.
These protocols provide a framework for recovery, but the real progress unfolds in the day-by-day and week-by-week adjustments.
Day-by-Day and Week-by-Week Checklist
Recovery is divided into three key phases, with peptide doses adapted for each stage:
| Phase | Timeline | BPC-157 Dose | TB-500 Dose | Goal |
|---|---|---|---|---|
| Acute / Loading | Days 1–14 | 500 mcg twice daily | 2.5–5 mg twice weekly | Reduce inflammation and kickstart angiogenesis |
| Proliferative / Maintenance | Weeks 3–8 | 250 mcg once daily | 2.5 mg once weekly | Promote tissue repair and collagen production |
| Remodeling | Weeks 9–16 | 250 mcg once daily | Discontinued | Support tissue maturation and functional recovery |
Safety and Follow-Up Recommendations
To ensure a safe recovery, follow these precautions:
- Monitor the incision site daily. Look for gradual healing with minimal redness. If the area becomes swollen, hot, or starts discharging, stop peptide therapy immediately and contact your surgeon. Peptides can speed up healing but won’t address infections.
- Track pain and range of motion (ROM). If ROM doesn’t improve as expected during physical therapy, reassess the protocol rather than increasing the dosage.
- Discontinue peptides if necessary. Stop treatment if there are signs of malignancy, infection, or significant setbacks in ROM.
Athletes should note that BPC-157 and TB-500 are prohibited by WADA (World Anti-Doping Agency) as of January 2022 and 2009, respectively. This should be a key consideration before starting any peptide protocol.
Lastly, proper nutrition is essential. Protein intake of 1.6–2.0 g/kg of body weight and 500–2,000 mg of Vitamin C daily provides the building blocks for collagen synthesis.
For more clinical guidance on peptide therapy, licensed healthcare professionals can visit PeptidePrescriber.
Documentation and Quality Assurance
When it comes to peptide therapy in post-surgical recovery, thorough documentation and quality assurance aren't just about meeting standards - they're key to ensuring patient safety and improving protocols over time. By keeping detailed records, practitioners can protect both their patients and themselves while paving the way for meaningful refinements.
Required Documentation
Every patient file should include critical details about the peptide source. Specifically, this means recording the 503A compounding pharmacy name, the lot number, and the Certificate of Analysis (COA) for each batch. The COA confirms essential factors like purity, sterility, potency, and endotoxin levels. Without these details, it's impossible to verify what was administered if complications arise.
In addition to sourcing information, dosing logs need to be just as detailed. They should include:
- The exact dose in micrograms (mcg) or milligrams (mg)
- Frequency and time of day for each dose
- The administration route (typically subcutaneous)
- Any co-administered therapies, such as NSAIDs, Vitamin C, Zinc, or collagen supplements, which can influence peptide activity.
It’s also crucial to log the reconstitution date for each peptide vial. Reconstituted peptides must be refrigerated and used within 28 days to maintain their efficacy. This level of detail is essential for tracking outcomes and making timely adjustments when needed.
Outcome Tracking and Adverse Event Reporting
Once proper documentation is in place, the next step is systematic tracking of outcomes. The table below highlights key metrics to monitor and how often they should be assessed:
| Metric Category | Specific Markers | Frequency |
|---|---|---|
| Wound Healing | Incision closure, redness, heat, discharge, scar texture | Daily |
| Functional Recovery | Range of Motion (ROM), PT milestones, return-to-activity dates | Weekly |
| Patient-Reported | Pain at rest, pain during movement, sleep quality | Daily |
| Adverse Events | Injection site reactions, dizziness, nausea, water retention | As needed at each occurrence |
| Lab/Biological | IGF-1, fasting glucose, fasting insulin (if using GH secretagogues) | Baseline & Weeks 8–12 |
Even minor adverse events, like localized warmth or bruising at the injection site, should be logged immediately. For systemic responses, such as dizziness or lethargy, it’s important to note the timing in relation to the dose. This information is vital for adjusting protocols and adhering to clinic reporting policies.
"The risk of returning to full activity before tissue has adequately matured is the same regardless of whether peptides were used. I use the same return-to-activity criteria for peptide-treated patients as for any other patient." - Dr. Julian Douwes
Ongoing Protocol Refinement
Patient outcomes are the foundation for refining protocols. By comparing each individual's recovery milestones with standard post-surgical benchmarks, practitioners can identify trends. For instance, if patients are reaching ROM and strength goals 1–3 weeks earlier than expected, that’s a valuable insight worth documenting. On the flip side, if progress slows, detailed records can help pinpoint whether the issue lies in dosing, sourcing, or patient compliance.
Given how fast the field of peptide therapy is evolving, staying informed is crucial. Resources like PeptidePrescriber offer healthcare professionals access to evidence-based protocols, regulatory updates, and compliance tools to stay ahead in this dynamic space.
Conclusion: Building a Reliable Post-Surgical Peptide Protocol
Creating a dependable post-surgical peptide protocol requires careful timing, precise combinations, and consistent clinical supervision. Initiating BPC-157 and TB-500 within 24–72 hours after surgery and aligning with the biological healing phases - Acute (Days 1–14), Proliferative (Weeks 3–8), and Remodeling (Weeks 9–16+) - ensures these peptides are used at their most effective points.
It’s important to emphasize that peptides are supplements to rehabilitation, not substitutes. Dr. Julian Douwes, M.D., underscores this distinction:
"Peptides cannot replace proper rehabilitation... The rehabilitation is the foundation. The peptides are the adjunct."
This guide outlines the essential steps to support each healing phase effectively.
Key practices like sourcing peptides from licensed 503A compounding pharmacies, maintaining detailed dosing records, and systematically tracking outcomes help establish reliable protocols and foster ongoing improvement.
For clinicians ready to adopt these protocols, PeptidePrescriber offers tools like evidence-based dosing protocols, reconstitution calculators, injection guides, regulatory information, and pharmacy-neutral sourcing strategies to move seamlessly from planning to compliant clinical application.
FAQs
How do I know when it’s safe to start peptides after surgery?
The timing of peptide therapy after surgery is a critical factor and should always be planned in collaboration with your surgical team. Typically, most guidelines suggest beginning therapy 24–72 hours after the operation, once the primary clot has stabilized. Starting too soon could interfere with clot formation, while waiting too long might mean missing the early stages of tissue repair. For specific surgeries, such as gastrointestinal or vascular procedures, a longer waiting period may be required. Always consult your surgeon before starting therapy to ensure it aligns with your recovery plan.
Which surgeries benefit most from BPC-157 vs TB-500?
BPC-157 and TB-500 are commonly paired to aid recovery after surgery, particularly for orthopedic, musculoskeletal, or significant internal procedures. BPC-157 focuses on localized healing, aiding soft-tissue repair, promoting angiogenesis (the formation of new blood vessels), and supporting tendon and ligament recovery. On the other hand, TB-500 offers systemic benefits by encouraging cell migration, reducing inflammation, and preventing the formation of stiff scar tissue. While BPC-157 is best suited for treating targeted injuries, TB-500 is more effective for addressing larger-scale injuries or surgeries involving muscles, ligaments, or fascia.
What side effects or red flags mean I should stop peptides?
If you notice symptoms like excessive redness, warmth, or discharge at the incision site, stop using peptides immediately and contact your surgeon. Discontinue their use if you experience any adverse reactions or health issues. Peptides should be avoided if you have active cancer, infections at the injury site, or are taking blood thinners - unless your doctor advises otherwise. Always keep your surgical team informed about any peptide use.