
Peptide therapy impacts your body in ways that aren’t always obvious, which is why lab testing is essential. It helps track progress, ensures safety, and informs treatment adjustments. Here's the key takeaway: Without lab tests, you’re guessing. Monitoring markers like IGF-1, glucose, and liver enzymes allows clinicians to fine-tune therapy and catch issues early.
Key Points:
- Baseline Tests: Includes CBC, CMP, fasting glucose, HbA1c, and IGF-1. These are done 2 weeks before starting therapy.
- Follow-Ups: Check progress at 6–8 weeks, focusing on safety markers like ALT/AST and glucose levels.
- Ongoing Monitoring: Every 3–6 months, with annual reviews for a full health check.
Lab testing isn’t just about tracking numbers - it’s about ensuring therapy works safely and effectively. If you’re considering peptide therapy, make sure lab monitoring is part of the plan.
The Emerging Science and Clinical Application of Peptide Therapy
General Framework for Lab Monitoring
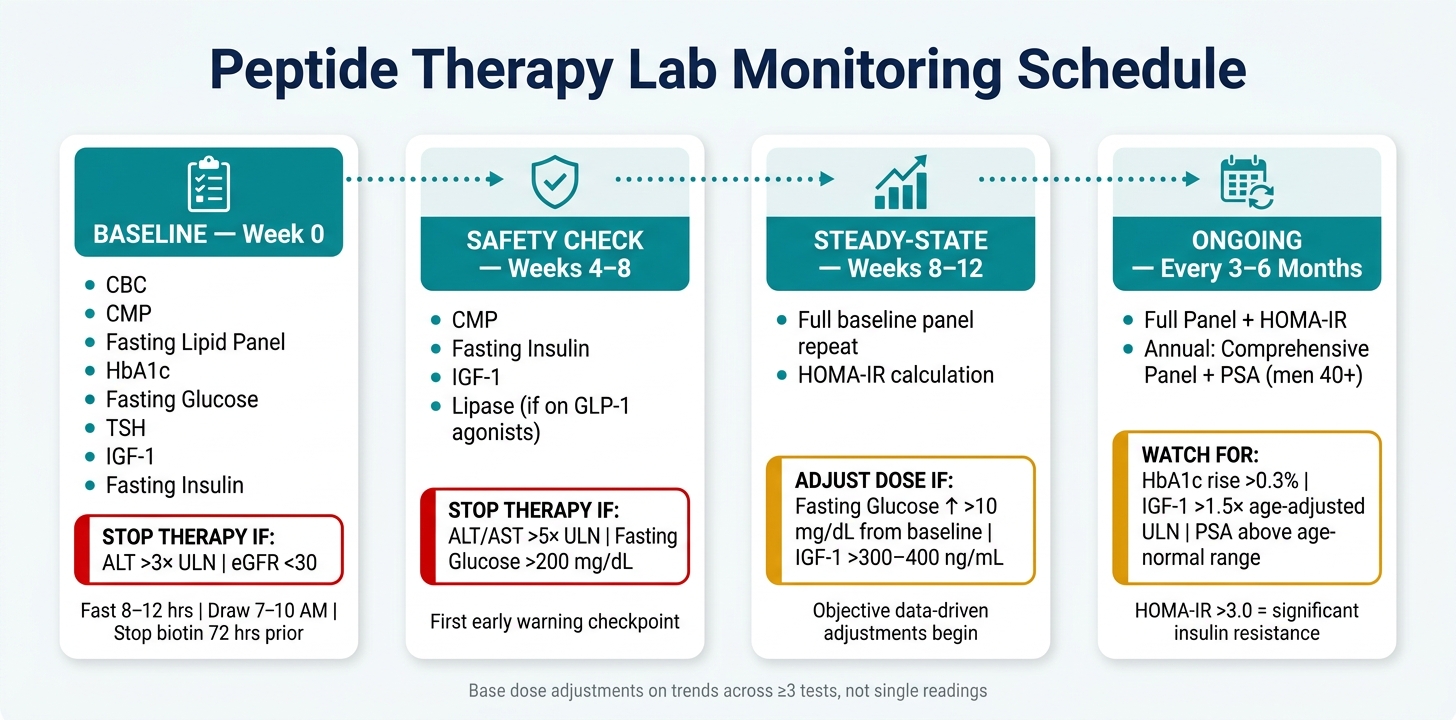
Peptide Therapy Lab Monitoring Schedule: Key Tests & Thresholds
Establishing a structured lab monitoring schedule is key to moving from reactive care to proactive management. This process should kick off even before the first dose of therapy.
Baseline Testing Before Starting Therapy
The first step is baseline testing, which provides a reference point for all future measurements. These tests need to be completed within two weeks before starting therapy.
The typical baseline panel includes:
- Complete Blood Count (CBC)
- Comprehensive Metabolic Panel (CMP)
- Fasting lipid panel
- HbA1c and fasting glucose
- Thyroid function tests (TSH)
- IGF-1
- Fasting insulin
These tests assess the metabolic, hepatic, renal, and hormonal systems - areas often influenced by peptide therapy. However, there are two critical red flags to watch for: an ALT level exceeding 3× the upper limit of normal and an eGFR below 30. Therapy should be paused if either is present, as continuing could pose significant risks.
"Without lab testing, you're flying blind, guessing at doses, and missing early warning signs that could prevent serious complications." - FormBlends
For accurate results, patients should fast for 8–12 hours before their blood draw and schedule the test between 7:00 AM and 10:00 AM to account for hormonal fluctuations. Additionally, biotin should be discontinued 72 hours before testing, as it can interfere with thyroid and hormone assays, leading to inaccurate readings.
Follow-Up Testing During Therapy
The first follow-up, usually between weeks 4 and 8, serves as a safety checkpoint. This phase focuses on identifying early warning signs. Key tests to repeat include the CMP, fasting insulin, and IGF-1. If the patient is on GLP-1 agonists like semaglutide or tirzepatide, a lipase test should be added to check for pancreatic stress.
A more comprehensive follow-up at week 12 provides a clearer picture of how the patient is responding to therapy. By this point, most peptides have begun to show measurable effects, enabling adjustments based on objective data rather than just patient feedback.
During active treatment, specific thresholds to watch for include:
- Fasting glucose increasing by more than 10 mg/dL from baseline during GH secretagogue therapy, which may require dose adjustments.
- ALT/AST levels exceeding 5× the upper limit of normal, which should prompt an immediate halt in therapy.
Ongoing monitoring ensures that any necessary adjustments are made early, reducing risks and improving outcomes.
Periodic Monitoring and Documentation
Once the patient stabilizes, testing should occur every 3–6 months, with an annual comprehensive review that includes a full panel recheck. For men over 40, this should also include a PSA test.
At each periodic review, calculating the HOMA-IR (using fasting glucose and insulin) is recommended. A value above 3.0 indicates significant insulin resistance, which is especially important for patients on MK-677. This therapy, due to its sustained GH elevation, carries a higher risk of insulin resistance compared to injectable secretagogues.
The table below summarizes the recommended monitoring schedule and key thresholds:
| Timeframe | Recommended Tests | Red Flag Thresholds |
|---|---|---|
| Baseline (Week 0) | CBC, CMP, Lipids, HbA1c, IGF-1, TSH, Fasting Insulin | ALT >3× ULN; eGFR <30 |
| Follow-Up (Weeks 4–8) | CMP, Fasting Insulin, IGF-1, Lipase (for GLP-1s) | ALT/AST >5× ULN; Fasting Glucose >200 mg/dL |
| Periodic (3–6 Months) | Full Baseline Panel + HOMA-IR | HbA1c rise >0.3%; IGF-1 >1.5× age-adjusted ULN |
| Annual | Comprehensive Panel + PSA (Men >40) | PSA rise above age-appropriate normal range |
When making dose adjustments, rely on trends observed across at least three tests to ensure accuracy and consistency.
Core Lab Tests for Peptide Therapy
These lab panels are essential for understanding how peptide therapy impacts key physiological systems. Since peptides often influence areas like liver function, kidney health, metabolism, blood composition, and hormones, these tests form the foundation for monitoring therapy effectively. Below are five critical panels that ensure therapy remains safe and effective.
Complete Blood Count (CBC)
The CBC provides insights into blood cell health, with hematocrit (HCT) being a crucial marker in peptide therapy. Growth hormone–releasing peptides (GHRPs) can elevate HCT levels, especially when combined with testosterone protocols. Clinically, an HCT above 52–54% often signals the need to pause therapy. Additionally, white blood cell (WBC) counts are monitored to detect immune responses or contamination risks.
Comprehensive Metabolic Panel (CMP)
The CMP evaluates liver enzymes, kidney function, glucose levels, and electrolytes, acting as a safety net. For example, an ALT level more than three times the upper limit of normal (ULN) is a critical warning sign. Patients using GLP-1 agonists like semaglutide should be monitored for potential kidney stress, as dehydration can lower eGFR. To avoid skewed results, patients should refrain from intense exercise 48 hours before testing, which can elevate AST and creatine kinase levels.
Fasting Lipid Panel
This panel measures total cholesterol, LDL, HDL, and triglycerides, offering insights into cardiovascular and metabolic health. Responses to peptides vary: GLP-1 agonists like tirzepatide often reduce triglycerides, while GH-axis peptides may temporarily raise LDL levels as the body adjusts. Monitoring trends across multiple tests is more reliable than a single result.
Glycemic Control Tests
Tests like fasting glucose, HbA1c, and fasting insulin provide a detailed picture of metabolic health. These are especially important for patients on GH secretagogues, as growth hormone can interfere with insulin function. For instance, MK-677 has been shown to increase fasting glucose by 15–20 mg/dL in clinical trials. For those on GLP-1 agonists, these tests confirm improvements in markers like HbA1c. Fasting insulin levels also allow for the calculation of HOMA-IR (Fasting Glucose × Fasting Insulin ÷ 405), with an optimal value being under 1.0.
Thyroid Function Tests
A full thyroid panel - including TSH, free T4, and free T3 - is critical because GH-axis peptides can affect the conversion of T4 to T3, potentially masking hypothyroidism. Undiagnosed thyroid issues can reduce the effectiveness of peptide therapy. Additionally, GLP-1 agonists carry a theoretical risk of thyroid C-cell hyperplasia, based on animal studies, making baseline thyroid screening a necessary precaution.
| Core Panel | Key Markers | Role in Peptide Therapy |
|---|---|---|
| CBC | HCT, WBC, Platelets | Identifies polycythemia and immune changes |
| CMP | ALT, AST, Creatinine, eGFR, Glucose | Tracks liver and kidney health |
| Lipid Panel | Total Cholesterol, LDL, HDL, Triglycerides | Monitors cardiovascular and metabolic shifts |
| Glycemic Panel | HbA1c, Fasting Glucose, Fasting Insulin | Evaluates glucose control and insulin sensitivity |
| Thyroid Panel | TSH, Free T4, Free T3 | Screens for thyroid dysfunction that may affect metabolism |
sbb-itb-7164bd9
Indication-Specific Lab Monitoring
Expanding on the general lab monitoring framework, this section delves into specific markers tailored to different peptide classes. These markers go beyond standard lab tests, offering insights that align with the peptide's unique mechanism of action. By incorporating these specifics into a monitoring plan, clinicians can better evaluate and adjust therapies.
Growth Hormone and IGF-1 Modulating Peptides
For peptides like CJC-1295, Ipamorelin, or Sermorelin, IGF-1 is the primary marker to track. It provides a reliable reflection of cumulative GH output and remains more stable in the bloodstream compared to GH itself. The goal is often an IGF-1 level within the 200–300 ng/mL range, ideally in the upper third of the age-adjusted reference range. Additionally, prolactin and cortisol levels should be monitored for peptides like GHRP-2 and GHRP-6, which may elevate these hormones.
Interpreting IGF-1 levels requires an age-based perspective. For instance, a reading of 250 ng/mL might be optimal for a younger adult but excessive for an older individual. If IGF-1 exceeds 300–400 ng/mL or fasting glucose increases by more than 20–25 mg/dL from baseline, reducing the dose may be necessary.
"A GH secretagogue protocol that doesn't check IGF-1 at 6–8 weeks isn't monitoring - it's hoping." – Peptidings
Metabolic and Weight-Loss Peptides
For GLP-1 agonists like semaglutide and tirzepatide, glycemic and lipid markers are essential. Clinical studies show that semaglutide (2.4 mg) can lower HbA1c by 0.5–1.5% in diabetic patients, while tirzepatide may achieve reductions of 1.0–2.4%. These therapies are also linked to triglyceride reductions of 15–35% and modest LDL decreases of 5–15%.
Monitoring amylase and lipase levels is critical to screen for pancreatitis. Therapy should be stopped if lipase exceeds three times the upper limit of normal, especially if accompanied by severe abdominal pain. Tracking body composition every 12 weeks - using DEXA scans or bioimpedance - can help ensure that weight loss primarily targets fat, not muscle.
Sexual Function and Reproductive Health Peptides
Peptides like PT-141 (bremelanotide) and kisspeptin analogs, which target sexual function and reproductive health, require a focused sex hormone panel. This includes total and free testosterone, estradiol, LH, FSH, and prolactin measured at baseline and during follow-up. Elevated prolactin is a key marker, as it can suppress testosterone and reduce libido.
For men, monitoring the estradiol-to-testosterone ratio is essential, as an imbalance can mimic low testosterone symptoms. For women, estradiol and progesterone levels should be interpreted in the context of their menstrual cycle or menopausal status to differentiate between natural fluctuations and therapy-induced changes.
Musculoskeletal and Recovery Peptides
Peptides like BPC-157 and TB-500, used for tissue repair and recovery, lack direct efficacy markers due to limited human studies. BPC-157 has been tested in only a few small trials, while TB-500 has no published human clinical data. Monitoring focuses on safety and indirect indicators.
Markers like hs-CRP and ESR can track systemic inflammation, with declining levels over 4–6 weeks suggesting potential anti-inflammatory effects. Functional outcomes, such as pain levels and range of motion, are also important to assess. Blood samples should be collected on rest days to avoid exercise-related interference with results.
Immune-Modulating and Anti-Inflammatory Peptides
Peptides like Thymosin Alpha-1 or low-dose naltrexone (LDN), used for immune modulation or chronic inflammation, require a broader inflammatory workup. Key tests include hs-CRP and a CBC with differential, while patients with autoimmune conditions may also need baseline autoantibody panels (e.g., ANA, anti-dsDNA, RF) to evaluate changes in immune activity.
| Peptide Class | Primary Efficacy Marker | Key Safety Markers |
|---|---|---|
| GH Secretagogues | IGF-1 | Fasting Glucose, Prolactin, PSA (men 40+) |
| GLP-1 Agonists | HbA1c, Fasting Glucose | Amylase, Lipase, eGFR, ALT/AST |
| Sexual/Reproductive Peptides | Testosterone, Estradiol, LH/FSH | Prolactin, SHBG |
| Recovery Peptides | hs-CRP, ESR (indirect) | CMP, CBC with differential |
| Immune-Modulating Peptides | hs-CRP, CBC with differential | Autoantibody panels (ANA, RF) |
When monitoring systemic inflammation, focus on trends over time rather than isolated data points.
Implementing Lab Monitoring in Clinical Practice
Integrating standardized lab monitoring protocols plays a key role in improving the effectiveness of peptide therapy. These steps help ensure that lab tests are used efficiently, as outlined in this checklist.
Setting Up Standardized Testing Protocols
To streamline lab monitoring, divide tests into two categories:
- Universal Panel: Includes CMP, CBC, lipids, HbA1c, and TSH for all patients.
- Add-on Panels: Tailored to specific peptide classes, such as IGF-1 for GH secretagogues, lipase for GLP-1 agonists, or a full sex hormone panel for reproductive peptides.
This approach minimizes unnecessary testing while ensuring nothing critical is overlooked.
Timing is key. Blood draws should be scheduled between 7:00 AM and 9:00 AM after an 8–12 hour fast to account for diurnal variations. For GH secretagogues, schedule the draw 12–24 hours after the last dose. For weekly GLP-1 agonists, aim for a mid-week trough just before the next dose.
Follow this timeline for lab assessments:
- Week 0: Baseline
- Weeks 4–6: Safety check
- Weeks 8–12: Steady-state
- Every 3–6 months thereafter: Ongoing monitoring
Before starting therapy, establish clear stop criteria in the patient’s chart. For example, document, “Stop therapy if weight loss is under 5 lbs within 16 weeks.” This avoids confusion when abnormalities arise and ensures decisions are based on predefined guidelines.
"The most irresponsible prescribing pattern in peptide medicine is straightforward: write the prescription, never mention labs, never follow up, refill when asked. This is not medicine. This is retail." – Peptidings
For those building workflows from scratch, resources like PeptidePrescriber offer tools such as consent templates and implementation checklists to help set up standardized monitoring protocols from day one.
Documentation and Trend Analysis
Rather than focusing solely on whether a result falls within population reference ranges, pay attention to how markers change compared to the patient’s baseline. For instance, an IGF-1 increase of 20–40% above baseline indicates that a GH secretagogue protocol is working. A single value like 250 ng/mL could mean very different things for a 35-year-old versus a 60-year-old, making age-adjusted interpretation essential.
To enhance tracking, use EHR flowsheets alongside patient symptom logs. Flowsheets allow you to quickly identify trends - like a marker moving in the wrong direction - that might be missed when reviewing individual visit notes. Additionally, incorporating a simple symptom log (e.g., rating sleep quality, energy, and gastrointestinal tolerance on a 1–10 scale) at each visit adds another layer of data to validate or question lab results.
"A monitoring program... is both a safety imperative and a practice-building asset - patients who receive systematic monitoring feel cared for, and the data generated allows practitioners to demonstrate objective improvements in biomarkers." – Peptide Association
Conclusion and Summary
Throughout this checklist, one thing is clear: consistent lab monitoring is the backbone of safe and effective peptide therapy. Making informed clinical decisions depends on objective lab data, not just how patients feel or report their progress.
The approach is simple yet critical: start with a baseline before initiating therapy, then stick to the recommended monitoring schedule. Some markers hold more importance depending on the protocol. For example, IGF-1 is the go-to marker for tracking the effectiveness of GH secretagogues. Meanwhile, HbA1c and fasting insulin help catch metabolic changes early, ALT/AST ensures liver health is on track, and specific markers like serum lipase for GLP-1 agonists address risks that general panels might overlook.
The financial burden is relatively low. A 22-marker baseline panel typically costs between $200 and $400. For uninsured patients, annual monitoring might run around $400 to $800. This is a small price to pay compared to the risks of overlooking critical warning signs, such as fasting glucose levels exceeding 126 mg/dL or ALT levels spiking to five times the normal upper limit.
By relying on objective lab data, clinicians can make timely therapy adjustments, improve patient safety, and ensure long-term success in their practice. To simplify this process, PeptidePrescriber (https://peptideprescriber.com) provides licensed prescribers with evidence-based tools, dosing protocols, and resources specifically tailored for peptide therapy.
Following these protocols ensures precise, timely interventions that maintain the highest standards of patient care.
FAQs
Which lab tests are essential before starting peptide therapy?
Before starting peptide therapy, setting a health baseline is an important step for proper dosing and monitoring. The following tests are commonly recommended:
- Comprehensive Metabolic Panel (CMP): Assesses liver and kidney health.
- Complete Blood Count (CBC): Provides an overview of overall blood health.
- Lipid and Thyroid Panels (TSH): Evaluates cholesterol levels and thyroid function.
For peptides targeting the growth hormone (GH) axis, it's essential to include IGF-1, fasting glucose, and HbA1c. If using GLP-1 agonists, focus on HbA1c, fasting glucose, and tests for kidney function.
How should I time fasting labs around my peptide dosing schedule?
For fasting lab tests like glucose, insulin, or lipid panels, it's important to fast for 10–12 hours, drinking only water during this time. Avoid coffee, especially if it contains cream or additives, as these can interfere with insulin levels. Aim to schedule your blood draw between 7:00 am and 9:00 am to align with the natural daily fluctuations of markers such as cortisol and testosterone. Additionally, stop taking biotin supplements at least 72 hours before the test to avoid any interference with the results.
What lab results mean I should pause or stop peptide therapy?
Peptide therapy might require a pause or discontinuation if follow-up lab results show significant deviations from baseline measurements. Here are some key markers to monitor:
- IGF-1 levels: If levels surpass 300 ng/mL, it could indicate the dosage is too high.
- Fasting glucose: An increase of 20–30 mg/dL above baseline may point to metabolic sensitivity.
- Hematocrit: Consistently elevated levels above 52–54% can be a concern.
- Liver enzymes or kidney markers: Any significant rise could suggest potential stress on these organs.
It’s crucial to address these changes promptly with input from a healthcare professional.