
For adult IM injections, I use a true 90-degree angle - every time. But that alone does not fix poor site choice or a needle that is too short. If the tip does not reach muscle, the dose can land in fat instead, which may slow absorption and increase local problems.
Here’s the short version:
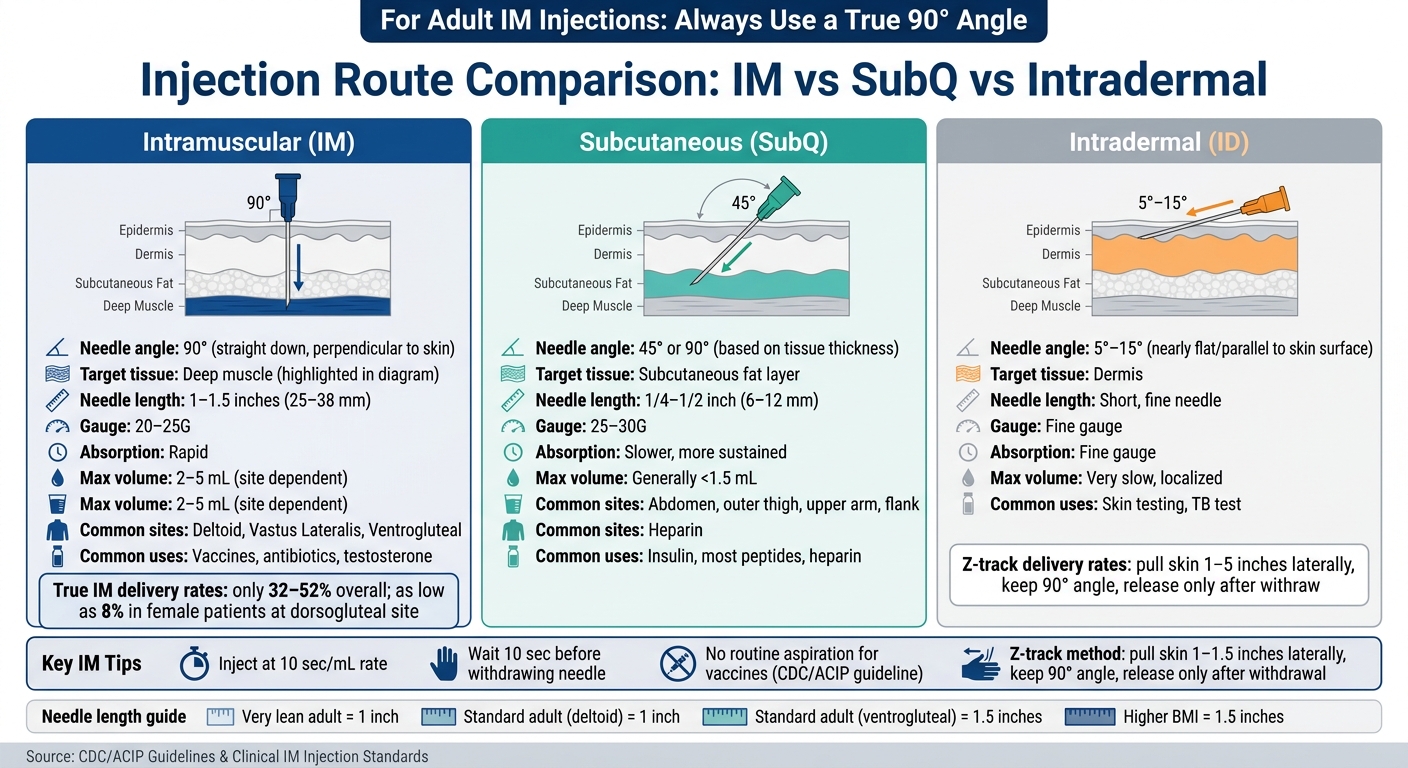
- IM = 90°
- Subcutaneous = usually 45° or 90°, based on tissue and needle (see subcutaneous injection technique)
- Intradermal = 5° to 15°
- Needle length matters as much as angle
- Main adult IM sites: deltoid, vastus lateralis, ventrogluteal
- Routine vaccine IM shots: no aspiration
- Z-track: keep the angle at 90°
- Reported true IM delivery rates: only 32% to 52% overall, and as low as 8% in female patients in some reports
What I take from this is simple: if you want the medication in muscle, you need the right angle, the right needle, and the right landmark. A straight-in approach works best when it matches the patient’s build and the injection site.
IM vs SubQ vs Intradermal Injection: Angle, Depth & Technique at a Glance
Types of Injection Angles » Intradermal, Subcutaneous, Intramuscular, Intravenous
sbb-itb-7164bd9
Quick Comparison
| Route | Angle | Target tissue | Usual needle length | Common use |
|---|---|---|---|---|
| IM | 90° | Muscle | 1 to 1.5 in | Vaccines, antibiotics, testosterone |
| SubQ | 45° or 90° | Fat layer | 1/4 to 1/2 in | Insulin, many peptides, heparin |
| Intradermal | 5° to 15° | Dermis | Short, fine needle | Skin testing |
In this guide, I focus on the parts that matter most in practice: 90-degree insertion, site selection, needle length, skin handling, Z-track use, no routine aspiration for vaccines, and patient-specific changes for kids, older adults, and higher-BMI patients, or when counseling patients on injection technique.
Why Injection Angle Matters in IM Administration
Angle decides whether the medication actually gets into the muscle. A true 90-degree insertion gives the needle the shortest path to that target. If the needle drifts even 10 to 15 degrees away from perpendicular, the tip can end up in subcutaneous tissue. In lean patients, it may also sit too close to the periosteum.
That matters because muscle is highly vascular, which is exactly why IM injections are meant to go there. Medication placed in muscle tends to absorb fast and evenly into systemic circulation, while also bypassing first-pass metabolism. If the dose ends up in subcutaneous tissue because the angle is off or the needle is too short, absorption slows down and local reactions are more likely.
What happens after the injection also depends on technique. Using the right angle, along with a slow injection rate of 10 seconds per mL, helps cut back on backflow along the needle track.
This same 90-degree standard applies across the main adult IM sites, but the landmarking shifts based on location. For deltoid, vastus lateralis, and ventrogluteal injections, perpendicular 90-degree insertion is the standard method. What changes from patient to patient is needle length, not angle. The site-specific sections below show how this works at the deltoid, vastus lateralis, and ventrogluteal sites.
1. Use a True 90-Degree Angle for Standard Adult IM Injections
A perpendicular, 90-degree insertion gives the needle the most direct path into the muscle belly. For standard adult IM injections, insert the needle straight in at 90 degrees.
Use a brisk, dart-like motion while stretching the skin taut with your non-dominant hand. That skin tension helps keep the needle path straight.
Once the needle is in, do a quick position check. A needle placed in muscle has little side-to-side movement. If it moves more freely, it may be in subcutaneous tissue.
Inject slowly, about 10 seconds per mL. Then wait 10 seconds before withdrawing the needle straight out, which can help reduce leakage.
A 90-degree angle still depends on using a needle length that can reach the muscle.
2. Match Needle Length and Gauge to Body Habitus
After angle, the next thing to get right is simple: can the needle actually reach the muscle?
Needle length determines whether a 90-degree injection reaches muscle. If the needle is too short, the medication may end up in subcutaneous fat no matter how good the angle or technique is.
For most adults, use a 1- to 1.5-inch needle (25-38 mm). The right choice depends on body size, injection site, and muscle depth. Patients with higher BMI often need a 1.5-inch needle so the needle can pass through the subcutaneous fat layer and reach muscle. In very lean adults, a 1-inch needle is usually enough. Go longer than needed, and the chance of hitting bone goes up.
The injection site matters too. The deltoid is closer to the surface, so a 1-inch needle is usually enough. The ventrogluteal and dorsogluteal sites sit deeper, which makes a 1.5-inch needle a more dependable pick for many patients. If bone is contacted, withdraw the needle about 0.4 inch (1 cm) before injecting.
Gauge affects flow and comfort, not depth. Most IM injections use 20-25G needles. Viscous medications often call for 20-21G, while aqueous solutions usually use 22-25G.
| Patient Habitus | Recommended Needle Length | Recommended Gauge |
|---|---|---|
| Very lean adult | 1 inch (25 mm) | 22-25G |
| Standard adult (deltoid) | 1 inch (25 mm) | 22-25G |
| Standard adult (ventrogluteal) | 1.5 inches (38 mm) | 22-25G |
| Higher BMI | 1.5 inches (38 mm) | 20-23G |
Once length and gauge are set, site landmarking determines where the needle should enter. Refer to our injection site guide for precise anatomical placement.
3. Choose the Correct Injection Site and Landmark Precisely
Next comes precise landmarking. A 90-degree angle only does its job when the needle enters the right spot. If the landmark is off, the injection can miss the muscle. That’s why careful landmarking matters so much.
Each site has its own method. This is also where many mistakes start: people skip palpation and rely on what the surface looks like.
- Deltoid: Find the acromion, then inject 2.5 to 5 cm below it in the center of the deltoid triangle.
- Ventrogluteal: Place the heel of the opposite hand on the greater trochanter, point the index finger toward the ASIS, and the middle finger toward the iliac crest. Inject in the center of the V.
- Vastus lateralis: Use the outer third of the middle third of the lateral thigh.
The ventrogluteal site gives you more room for error because subcutaneous tissue is thin there and the muscle is usually easy to rely on.
The best site also depends on the patient. The deltoid is the standard choice for vaccines and small-volume injections in adults, usually ≤1 mL. The vastus lateralis is the main site for infants and also works well for adults doing self-injection. The ventrogluteal site is the safest option for adults and children older than 7 months. It’s also a smart pick for older or lean patients, where muscle atrophy can make other sites less dependable. By contrast, the dorsogluteal site should be avoided for routine injections because it sits close to the sciatic nerve and major blood vessels.
| Site | Best For | Key Landmark |
|---|---|---|
| Deltoid | Adult vaccines, small-volume injections | 2.5–5 cm below the acromion process |
| Ventrogluteal | Adults, children >7 months, lean/older adults | Triangle between greater trochanter, ASIS, and iliac crest |
| Vastus Lateralis | Infants, self-injectors | Outer third of the middle third of the lateral thigh |
| Dorsogluteal | Less preferred; avoid when possible | Upper outer quadrant of the buttock |
Palpate the landmarks before every injection. Don’t trust surface appearance alone, especially in patients with a higher BMI.
Once you’ve mapped the site, keep the limb steady so the needle path stays on track.
4. Maintain Skin Tension and Stable Patient Positioning
Once you've marked the site, the next job is control. You want the needle to travel on a true 90-degree path into the muscle, and that starts with skin tension.
Use your non-dominant hand to stretch the skin taut. That firms up the surface and helps support a straight 90-degree entry.
For very lean patients or infants, do the opposite. Instead of stretching the skin, gently pinch or bunch the tissue. That adds a bit more space between the skin and bone and helps keep the needle tip in the muscle.
Patient position matters just as much. The target muscle should be relaxed before insertion. A tense muscle creates more resistance and usually means more pain. For the vastus lateralis, place the patient supine with the knees slightly bent. For the ventrogluteal site, side-lying or supine with the knees flexed works best.
Keep the syringe steady with the non-dominant hand so it doesn't shift during insertion.
Skin handling and positioning change a little by site:
| Injection Site | Recommended Position | Skin Technique |
|---|---|---|
| Deltoid | Arm relaxed at the side | Stretch skin; bunch for very thin patients |
| Vastus Lateralis | Supine, knees slightly bent | Stretch skin; bunch for infants/toddlers |
| Ventrogluteal | Side-lying or supine with flexed knees | Stretch skin |
5. Use the Z-Track Method When Clinically Indicated
Some medications are more irritating or more likely to leak after an IM injection. In those cases, the Z-track method can help keep the medication in the muscle without changing the injection angle. With this method, you pull the skin and subcutaneous tissue 1 to 1.5 inches (2.5 to 3.8 cm) away from the injection line before inserting the needle.
Keep that tissue displaced during the entire injection. Then release it only after the needle has been fully withdrawn. That shift creates a zigzag path that helps seal the medication in the muscle and cut leakage into the subcutaneous tissue.
The angle stays the same: 90 degrees. The goal here isn't to change your approach. It's to improve containment while keeping the tissue steady.
Use Z-track for irritating, oily, or viscous medications, including certain hormones, iron preparations, and benzathine penicillin. Once you've confirmed that Z-track is the right choice, keep the angle at 90 degrees and pay close attention to tissue stabilization.
After you withdraw the needle, apply gentle gauze pressure for 30 to 60 seconds. Do not massage the site.
Site selection also plays a big part when you need deeper muscle delivery and less backflow. Ventrogluteal injections often work well with Z-track because that site usually has thicker muscle and less subcutaneous tissue. When you need a straighter path into muscle and less leakage into subcutaneous tissue, Z-track is often a good fit.
6. Avoid Routine Aspiration for Most Vaccine IM Injections
The injection angle doesn't change, but one part of vaccine IM technique has. Routine aspiration is no longer part of vaccine injections. Aspiration means pulling back on the plunger to check for blood. That used to be standard practice. Now, the CDC and the Advisory Committee on Immunization Practices (ACIP) do not recommend it for IM vaccine injections.
Why the change? These vaccine injection sites carry a low risk of intravascular injection, so aspiration adds little. For routine vaccines, do not aspirate. Use steady pressure on the plunger, give the injection, and remove the needle right away. No pause. No pull-back.
There is one limit to that rule. It applies to routine vaccines, not to every IM medication. Aspiration should be reserved for select nonvaccine IM medications when the dorsogluteal site is used.
Also, after skin prep, let the alcohol dry for 45–60 seconds before injecting.
7. Adjust Technique for Pediatrics, Older Adults, and Higher-BMI Patients
Patient anatomy affects needle length, site choice, and how you handle the skin. The injection angle still stays at 90 degrees. What changes is tissue depth and how far the needle needs to go to reach muscle.
For pediatric patients, needle length depends on age and body size. A 1-inch needle is standard for infant thigh injections, while children 3 years and older may need 1 to 1.25 inches, depending on size. For infants, use a 22–25 mm needle when bunching the tissue, or a 16 mm needle when stretching the skin flat.
For older adults with reduced muscle mass, the main concern is the needle hitting bone. Gently bunch the tissue before insertion so the medication reaches muscle instead of going too deep.
For patients with higher BMI, standard needles may not reach muscle. A 1.5-inch needle is usually needed for deltoid injections in women over 200 lbs or men over 260 lbs. In many cases, the ventrogluteal site is the better pick because it has thin subcutaneous tissue and a thick gluteus medius.
These population-based changes should be built into prescriber protocols and quick-reference tools. When anatomy shifts the usual approach, use this table:
| Population | Preferred Site | Needle Length | Max Volume |
|---|---|---|---|
| Infants (<3 yrs) | Vastus Lateralis | 1 inch | 0.5–1 mL |
| Children (3–10 yrs) | Vastus Lateralis / Deltoid | 1–1.25 inches | 1 mL |
| Older Adults With Reduced Muscle Mass | Ventrogluteal | 5/8–1 inch | 2 mL |
| Adults With Higher BMI (Women over 200 lbs / Men over 260 lbs) | Ventrogluteal | 1.5 inches | 3 mL |
8. Standardize and Document IM Angle Technique in Clinical Practice
Consistent IM technique starts with a written protocol. Once your team sets the angle and needle length, document them the same way every time. If that step gets skipped, people tend to fall back on personal habits. That’s where technique starts to drift.
Written standards make correct technique part of daily practice instead of something left to memory.
A solid protocol should spell out the basics:
- a true 90-degree insertion angle
- site selection based on age, muscle mass, and injection volume
- needle length matched to body habitus, BMI, age, and sex
- Z-track use when indicated
Documentation should match the technique used, and it should line up with the Rights of Medication Administration. Each injection record should include the exact muscle, side, and landmarks used. For example, write “right ventrogluteal site” instead of “buttock.” It should also include the needle gauge and length, the technique used, and any immediate patient response.
Use the table below as a minimum documentation standard:
| Documentation Element | What to Record | Why It Matters |
|---|---|---|
| Injection Site | Specific muscle and side (e.g., left ventrogluteal site) | Supports site rotation and follow-up |
| Technique | 90-degree angle, Z-track, skin stretching or bunching | Confirms adherence to the written protocol |
| Equipment | Needle gauge and length (e.g., 22G, 1.5 inch) | Helps verify that the medication reached the muscle |
| Patient Response | Pain level, bleeding, or immediate adverse reactions | Supports follow-up and complication tracking |
PeptidePrescriber offers injection guides and clinical tools for protocol standardization.
Site-Specific Angle Guidance for Common IM Injection Locations
For IM injections, the needle goes in at 90 degrees at every site. That part doesn't change. What does change is the landmark and the depth needed to reach muscle.
Put simply: the angle stays fixed, but the room for error doesn't. Use the same straight-in entry each time, then match your landmarking and needle depth to the anatomy at that site.
Deltoid: 90-Degree Insertion With Upper-Arm Landmarking
The deltoid is the standard site for adult vaccines and small-volume medications. Find the acromion process, then measure 1 to 2 inches (2.5 to 5 cm) below it. The injection should go into the center of that triangular muscle mass at a true 90-degree angle to the skin.
The main limit here is volume. Deltoid injections should be 1 mL or less.
Vastus Lateralis: 90-Degree Insertion With Lower Risk of Vascular or Nerve Injury
The vastus lateralis sits along the outer thigh and is easy to landmark. It also carries a low risk of striking major nerves or blood vessels. To find it, divide the outer thigh into thirds between the greater trochanter of the femur and the lateral femoral condyle of the knee. The injection goes into the middle third of that outer anterolateral area.
This site can take up to 5 mL in adults, which makes it a good option when the arm or gluteal sites don't fit the situation.
Ventrogluteal: 90-Degree Insertion With Reliable Muscle Depth
To landmark the ventrogluteal site, place the heel of your hand on the patient's greater trochanter, point your index finger toward the anterior superior iliac spine (ASIS), and spread your middle finger toward the iliac crest. The injection site is in the center of the "V" made by those fingers.
This site can handle up to 5 mL and works well for larger-volume or more irritating medications.
In current U.S. practice, this is widely viewed as the safest routine IM site. That's because the subcutaneous layer is thin, the gluteus medius muscle is thick, and the muscle depth tends to stay more consistent across body types.
Dorsogluteal: Less Preferred in Current U.S. Practice
The dorsogluteal site, once marked as the upper outer quadrant of the buttock, is now used less often in U.S. practice. One big issue is that true intramuscular delivery is inconsistent. Reported rates range from 32% to 52% overall, and drop as low as 8% in female patients.
There's also a safety concern. The sciatic nerve and major blood vessels are close to this area, and nearly 90% of patients with a sciatic nerve injury from a dorsogluteal injection present with an immediate foot drop.
Here's a quick side-by-side reference for site, landmark, and volume:
| Site | Landmark Reference | Max Volume |
|---|---|---|
| Deltoid | 2.5–5 cm below the acromion process | ≤ 1 mL |
| Vastus Lateralis | Middle third of outer thigh (greater trochanter to lateral femoral condyle) | 1–5 mL |
| Ventrogluteal | Center of "V" formed by index finger (ASIS) and middle finger (iliac crest) | 1–5 mL |
| Dorsogluteal | Upper outer quadrant of buttock | 1–5 mL |
Special Population Considerations
Sometimes angle isn't the issue. Needle length and site selection are what need to change.
Patient anatomy affects how deep you need to go and where you should inject. But the injection angle stays the same: 90 degrees.
Infants and Young Children
In kids, muscle depth changes fast with age. That's why site choice comes first.
Use the vastus lateralis for neonates, infants, and toddlers. As children get older and build more muscle mass, shift to the deltoid.
Very Lean Adults
For very lean adults, use a 1-inch needle in the deltoid. A 5/8-inch needle should be kept for cases where the skin is stretched tight and there is very little subcutaneous tissue.
Older Adults With Reduced Muscle Mass
In older adults, muscle loss can make some sites less dependable and can bring bone closer to the surface.
Use the ventrogluteal site when muscle mass is reduced. Stretch the skin flat, and go with a shorter needle only when tissue depth is clearly limited.
Patients With Higher BMI
For many larger adults, a 1.5-inch needle is the better choice because a 1-inch needle may not reach the muscle.
For women over 200 lbs (90 kg) and men over 260 lbs (118 kg), a 1.5-inch (38 mm) needle is typically required. The angle does not change. Keep it at 90 degrees and use a longer needle to reach muscle.
Clinical Tools and Training Support for Peptide Prescribers
Good IM technique comes down to three things: clear written protocols, staff training, and quick-reference tools.
Build Injection Technique Into Written Protocols
A written protocol cuts down on guesswork and helps everyone use the same method.
Your IM protocol should spell out:
- Needle length by body habitus: Match needle length to the patient’s size and the injection site so the medication reaches muscle
- Z-track indications: Use the Z-track method for oily, viscous, or irritating solutions
- Competency check: Require a short skills review when onboarding new staff or when adding a new injection site or medication
A short reference sheet can make those rules easier to use in day-to-day practice.
Use Reference Tools to Reduce Technique Variation
Onboarding and refresher training tend to work best when staff are using the same written standard.
PeptidePrescriber offers licensed healthcare professionals clinical tools, including injection guides, dosing protocols, and regulatory references. These resources can help reduce technique variation across staff.
IM vs. Subcutaneous Injection Angle: Quick-Reference Table
After you choose the site, use this table to double-check the route and insertion angle. For peptide prescribers, it gives a fast side-by-side look at the two routes used most often in practice.
Angle, Depth, and Common Uses at a Glance
IM injections use a 90° angle to reach muscle. SubQ injections use 45° or 90°, based on tissue thickness and needle length.
| Feature | Intramuscular (IM) | Subcutaneous (SubQ) |
|---|---|---|
| Insertion angle | 90° | 45° or 90° (based on tissue thickness) |
| Target tissue | Deep muscle | Subcutaneous tissue |
| Typical needle length | 1–1.5 in (25–38 mm) | 1/4–1/2 in (6–12 mm) |
| Typical gauge | 20–25 gauge | 25–30 gauge |
| Absorption rate | Rapid | Slower, more sustained |
| Max volume (adult) | 2–5 mL (site dependent) | Generally < 1.5 mL |
| Typical medications | Vaccines, antibiotics, testosterone, epinephrine | Insulin, most peptides, heparin |
| Common sites | Deltoid, vastus lateralis, ventrogluteal | Abdomen, outer thigh, upper arm, flank |
Most peptides are given SubQ. Use IM when the drug or protocol calls for faster systemic delivery.
Getting the route and angle right helps lower the chance of placing the injection into the wrong tissue layer.
Conclusion
For the deltoid, vastus lateralis, and ventrogluteal sites, the main rule doesn't change: a true 90-degree angle is the standard for adult IM injections. It gives the needle the most direct route into the muscle.
But angle is just one part of the picture. Needle length, injection site, and patient habitus all affect whether the medication actually reaches muscle. Those are the variables clinics should standardize in their protocols.
Safe IM delivery comes down to steady technique and patient-specific judgment. For clinics putting written IM protocols in place, PeptidePrescriber offers clinical tools, injection guides, and dosing protocols.
FAQs
How do I know if the needle actually reached muscle?
If the needle has reached muscle, it should have limited side-to-side movement. That’s different from subcutaneous tissue, which usually feels looser.
Proper site selection and the right anatomical landmarks help the needle reach the muscle while avoiding nerves and blood vessels. If you hit bone, the needle went too deep. Withdraw it about 1 cm.
Which IM site is safest for most adults?
The ventrogluteal site is generally seen as the safest intramuscular injection site for most adults. It’s often the first choice because the muscle is thick and sits away from major nerves and blood vessels.
The vastus lateralis and deltoid are also common injection sites. By contrast, the dorsogluteal site is usually discouraged because it lies too close to the sciatic nerve.
When should I use a 1-inch vs. 1.5-inch needle?
The right needle length comes down to body composition, weight, and the injection site.
A 1-inch (25 mm) needle is usually enough for:
- Adult men who weigh 130 to 260 lbs
- Adult women who weigh 130 to 200 lbs
A 1.5-inch (38 mm) needle is often used if:
- A woman weighs over 200 lbs
- A man weighs over 260 lbs
Smaller needles are often used for thinner individuals or for certain pediatric sites.