
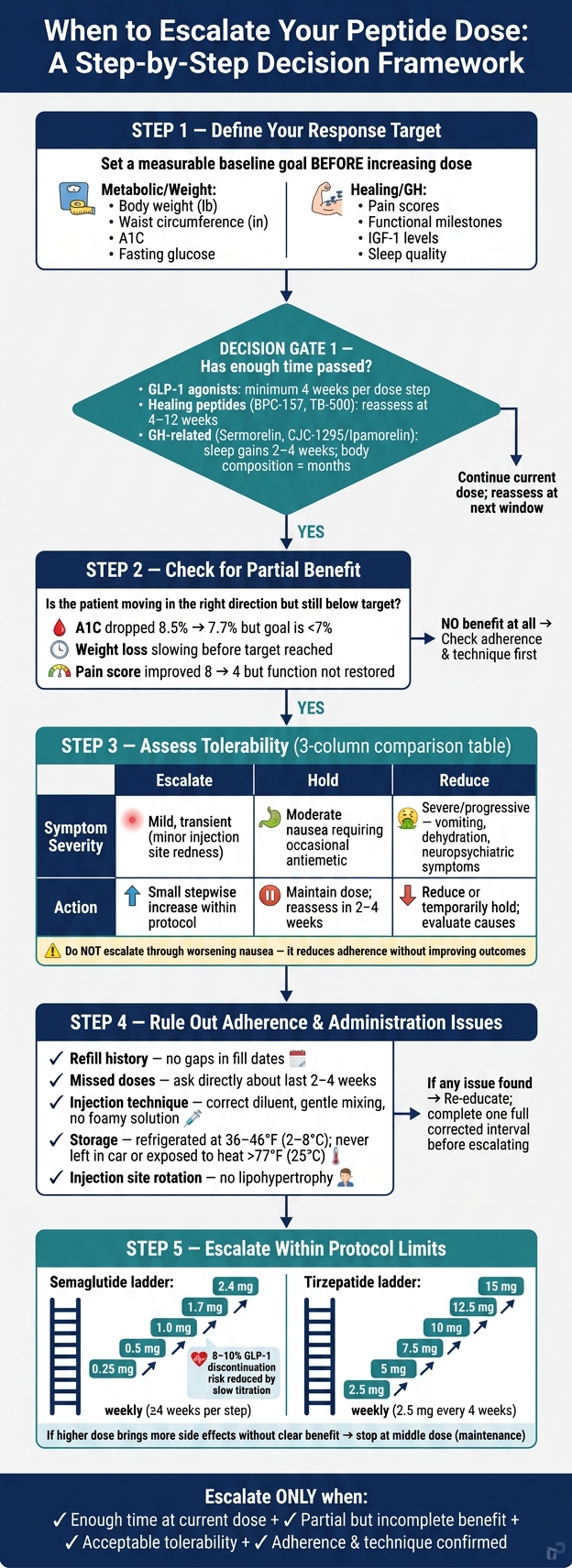
A higher peptide dose only makes sense when the current dose has had enough time, the patient has shown some response, and use has been consistent. If doses are being missed, injection technique is off, or side effects are getting worse, moving up too soon can backfire.
Here’s the short version:
- Don’t escalate by the calendar alone
- Set a clear target first like weight, waist size, A1C, fasting glucose, pain, or function
- Separate slow early progress from a true plateau
- Look for partial benefit, not just all-or-nothing results
- Hold or reduce if side effects are getting in the way
- Check missed doses, mixing, storage, and injection sites before changing anything
- Stay inside protocol limits for step size and timing
A few numbers help frame the decision:
- GLP-1 dose steps are often spaced by at least 4 weeks
- Semaglutide may move from 0.25 mg to 2.4 mg weekly in set steps
- Tirzepatide often increases by 2.5 mg every 4 weeks, up to 15 mg weekly
- GLP-1 users losing about 1–2 lb/week usually do not need a higher dose just because one is available
- GI-related drop-off with GLP-1 therapy is about 8%–10%
If I had to boil the article down to one rule, it would be this: escalate only after time, response, tolerance, and correct use all line up. That keeps dose changes tied to patient progress instead of guesswork.
Peptide Dose Escalation Decision Framework
Retatrutide Masterclass: How To Use It Optimally (Dose, Frequency, Diet, Exercise, & Supplements)
sbb-itb-7164bd9
Define Response Before Increasing the Dose
Dose escalation should start with a clear response target, not a general feeling that things are moving too slowly. Before you increase the dose, pin down one thing first: what counts as a meaningful response for this patient? Set that at baseline, define the target threshold, and choose a follow-up metric you can track over time.
Use measures that fit the indication. For metabolic and weight-loss peptides, track:
- Body weight in lb
- Waist circumference in inches
- A1C
- fasting glucose
For healing-focused peptides, use pain scores and functional milestones. And don’t lean too hard on one data point. Trends matter more than single readings because fluid shifts, recent meals, and normal day-to-day swings can throw off the picture. Once response is defined, the next step gets much easier: sort out delayed onset from a real plateau.
Separate Early Lag Time From a True Response Plateau
A slow start doesn’t automatically mean the peptide isn’t working. With GLP-1s, early titration is mainly about tolerability, not maximum effect. In many cases, meaningful benefit shows up after dose escalation and can keep building for months.
A true response plateau means the patient has had enough time at a stable dose and the outcome trend has actually flattened. Early lag time is different. It simply means the peptide hasn’t had enough exposure yet to show its full effect.
Match reassessment to the peptide’s expected onset window instead of reacting out of frustration. For shorter-acting healing peptides, reassessment may make sense within 4–12 weeks, depending on the goal. For growth hormone–related peptides like sermorelin, sleep quality gains can show up within 2–4 weeks, while body composition changes may take months.
If the timeline fits and the benefit is still incomplete, the next step is to check whether tolerance or adherence is holding things back.
Look for Partial Benefit, Not Just No Effect
Partial benefit is often the strongest sign that escalation may help. It suggests the peptide is hitting its target, but the patient may not have reached the therapeutic threshold yet.
That can look like fasting glucose coming down but still sitting above goal, weight loss slowing before the target is met, or pain improving and then stalling short of the patient’s functional goals. Dose-response data support escalation when benefit is present but incomplete. If the patient is moving in the right direction, still sits meaningfully below target, and side effects remain manageable, a planned dose increase is a sensible next move.
Partial response leads straight to the next check: confirm side effects and dosing accuracy before escalating.
Check Tolerability and Adherence Before Raising the Dose
If the patient is getting some benefit and the timing makes sense, pause before moving the dose up. First, check tolerability and adherence. If one of those is off, deal with that first. If both look good, a dose increase is easier to justify.
Use Side Effect Burden to Decide Whether to Escalate, Hold, or Reduce
A dose is generally well tolerated when side effects are mild, expected, and not pointing to a safety problem. With injectable peptides, that often means mild nausea that fades, slight injection site irritation, or mild fatigue that clears over days to weeks. What matters most isn't just whether the patient notices symptoms. It's whether those symptoms interfere with daily life or make it harder to stay on treatment.
Do not escalate through worsening nausea; it reduces adherence without improving outcomes.
| Escalation Appropriate | Hold Current Dose | Reduce Dose | |
|---|---|---|---|
| Symptom Severity | Mild, transient (e.g., minor injection site redness); no impact on work, sleep, or adherence | Moderate (e.g., nausea requiring occasional antiemetic); symptoms controlled but not fully resolved | Severe or progressive (e.g., recurrent vomiting, dehydration risk, new neuropsychiatric symptoms, or injection site reactions suggesting allergy or infection) |
| Recommended Action | Consider a small, stepwise dose increase within protocol limits; provide anticipatory guidance on what to expect | Maintain current dose; optimize supportive care and reassess in 2–4 weeks before any further escalation | Reduce or temporarily hold; evaluate for alternative causes and document the adverse event if warranted |
For GLP-1–based therapies, there’s another guardrail. If a patient is already losing about 1–2 lb/week, guidance says not to keep pushing the dose higher just because a higher dose exists. The aim is steady progress, not the top dose on paper.
Poor tolerance and poor adherence often show up together. If you ease the side effects, adherence may improve without any dose increase. Once tolerability looks acceptable, the next step is to check whether missed doses, poor technique, or storage problems are behind the weak response.
Rule Out Missed Doses, Technique Errors, and Storage Problems
Before escalating, make sure the patient is actually getting the full intended dose. A weak response often comes down to imperfect adherence, and that review should happen before any dose change.
Start with refill timing. Compare the expected refill date with the actual fill history and look for gaps. Then ask a direct question: how many doses were missed in the last 2–4 weeks? With weekly injectables, even a small lapse during travel or a hectic stretch can dull the response.
Next, look at technique. Go through the full prep and injection process step by step. Small mistakes can add up fast. Misreading syringe markings, using the wrong diluent volume, mixing too roughly, or picking the wrong diluent can all cut exposure. Injection site rotation matters too. Using the same spot again and again can lead to lipohypertrophy, which may impair absorption even if everything else looks right.
Storage is the last big check. Peptides that need refrigeration should stay at 36–46°F (2–8°C). Time spent above 77°F (25°C), direct sunlight, or repeated freeze-thaw cycles can reduce potency even if the solution still appears clear. Ask plain, practical questions. Was it left in a car? In checked luggage? Out overnight? If storage looks questionable, replace the vial and reassess before changing the dose.
This table helps separate a true low pharmacologic response from one caused by adherence or administration problems:
| Clinical Clue | True Low Response | Likely Adherence or Administration Issue |
|---|---|---|
| Refill History | Consistent, on-time refills | Gaps in refill dates or unused medication remaining in the vial |
| Patient Logs | Documented doses matching prescribed schedule | Missing entries, reports of missed doses during travel or busy periods |
| Preparation | Correct diluent volume, gentle mixing, clear solution | Wrong diluent, aggressive shaking, cloudy or foamy solution |
| Storage | Refrigerated consistently at 36–46°F | Left at room temperature, in a car, or exposed to heat or light |
| Injection Site | Healthy tissue with regular site rotation | Lipohypertrophy, bruising, or consistent use of a single site |
| Next Step | Consider protocol-based dose escalation | Re-educate on technique and storage; defer escalation until one full corrected interval is completed |
Clinical tools such as injection guides, reconstitution calculators, and dosing checklists - including those on PeptidePrescriber - can make these reviews more consistent, especially for prescribers setting up a peptide practice. If the response is still low after these checks, move to protocol-based escalation.
Clinical Scenarios Where Escalation Makes Sense
Once the basics are in place, the next move is to match the response pattern to the peptide class.
Escalation Examples: GLP-1, Healing, and GH-Related Peptides
The same idea plays out a bit differently depending on the use case.
For weekly GLP-1 agonists like semaglutide or tirzepatide, escalation makes sense when the response is only partial after at least 4 weeks at a dose the patient can tolerate. For example, an A1C drop from 8.5% to 7.7% is progress, but it still leaves room to move up. The same goes for a patient who is losing weight at a steady pace but is still above goal on a tolerated semaglutide dose. Weight loss can keep going after a dose increase, so an early partial response doesn't mean the ceiling has been reached.
For healing peptides like BPC-157 or TB-500, the main sign is a plateau in pain or function. Say a patient's pain score falls from 8 to 4 on a visual analog scale in the first few weeks, then stays at 4 for two or more back-to-back assessments, with pre-injury function still out of reach. That's a stall worth looking at. Before moving the dose, make sure rehab is on track, nutrition is solid, and no co-factors, like poorly controlled diabetes, are getting in the way of healing. If those pieces check out and the protocol allows a higher dose, a small step up is reasonable.
For GH-related peptides like CJC-1295/Ipamorelin, escalation fits when IGF-1 has moved up from baseline but is still below target, and the patient reports only partial gains in energy, sleep quality, or body composition after 4–8 weeks at the starting dose. Do not push the dose past the IGF-1 target or through edema, joint stiffness, or carpal tunnel symptoms.
Escalate in Steps Without Exceeding Protocol Limits
Even when a dose increase makes sense, the change still needs to stay inside protocol-set steps and ceilings.
Dose changes should follow the stated step sizes and timing, not a faster is better mindset. For semaglutide-based weight-management protocols, that means moving through 0.25 mg → 0.5 mg → 1.0 mg → 1.7 mg → 2.4 mg weekly, with at least 4 weeks at each step. For tirzepatide, the schedule is 2.5 mg increases every 4 weeks, up to a maximum of 15 mg weekly. Starting low and holding each step for 4 weeks is the main way to cut GI-related discontinuation risk, which affects about 8%–10% of patients on GLP-1 therapies.
If a higher dose brings more side effects without a clear upside, stop at the middle dose. In many cases, that becomes the maintenance dose.
Use Structured Protocols and Key Decision Points
Once you’ve checked response, tolerance, and adherence, use a protocol to guide the escalation decision. That keeps the process repeatable, consistent, and easy to review later.
Before entering any dose change, document the key details:
- The indication
- The current dose
- Time at dose
- The target metric
- The response trend
- The reason for holding, escalating, or reducing
Those details should be in place before the change is entered.
Calculators and monographs help turn protocol steps into exact volumes and titration increments. When prescribers use shared tools, the workflow stays more consistent across the team.
PeptidePrescriber gives licensed healthcare professionals access to peptide monographs, dosing protocols, calculators, injection guides, regulatory references, and a prescriber network.
Conclusion: Key Points for Safe Dose Escalation
Escalate only after enough time at the current dose, partial but incomplete benefit, acceptable tolerability, and a negative adherence or administration check. Keep each increase within protocol step sizes and document the reason for the change.
FAQs
How do I tell a slow start from a true plateau?
Track the patient against clear baseline endpoints from the start. Some patients begin slowly, then pick up once steady-state levels are in place. For many peptides, that can happen at about four weeks.
Before you label the response a plateau, make sure the patient followed the protocol closely. That includes details like fasting requirements for growth hormone secretagogues, which can affect results more than people think.
If outcomes still haven't changed by the planned review point and adherence was solid, the plateau may be real. At that stage, a dose change or a shift in strategy may make sense.
What should I check before increasing the dose?
Before you increase a peptide dose, first make sure the patient is actually following the plan as prescribed. That includes when they take it, whether they’re meeting any fasting rules, and whether they’ve stayed on the current dose long enough to judge how it’s working.
You’ll also want to check recent lab markers, such as IGF-1, metabolic panels, or HbA1c. Then take a second look at the reason for the dose increase and confirm it still makes sense. At the same time, rule out any new contraindications or side effects that the patient can’t manage.
When should I hold or reduce instead of escalating?
Hold or lower the dose if the patient has intolerable side effects, such as ongoing gastrointestinal discomfort or nausea, or if they can’t handle higher maintenance doses.
Also review contraindications, including pancreatitis or other relevant medical history. Before moving the dose up, confirm adherence and check baseline health markers. A weak response may come from those issues, not from a dose that’s too low.